A good over-the-counter sleep aid is not the bottle that looks strongest on the shelf. It is the one that matches the way you are not sleeping, the length of time this has been going on, and the risks you personally bring to the decision. That sounds fussy until you are choosing between ZzzQuil, Benadryl, Unisom SleepTabs, melatonin gummies, magnesium, L-theanine, and valerian at 10:47 p.m.
The latest evidence does not support one universal winner. A 2025 scoping review of 51 randomized controlled trials found that melatonin and valerian had the strongest evidence for effectiveness and safety among OTC products for insomnia, but that does not mean either is the right answer for every bad night.[1] Antihistamines such as diphenhydramine and doxylamine can be more sedating in the short term. They also create the most common consumer mistake: treating “stronger” as automatically better.
Start With Three Questions Before You Pick an Ingredient
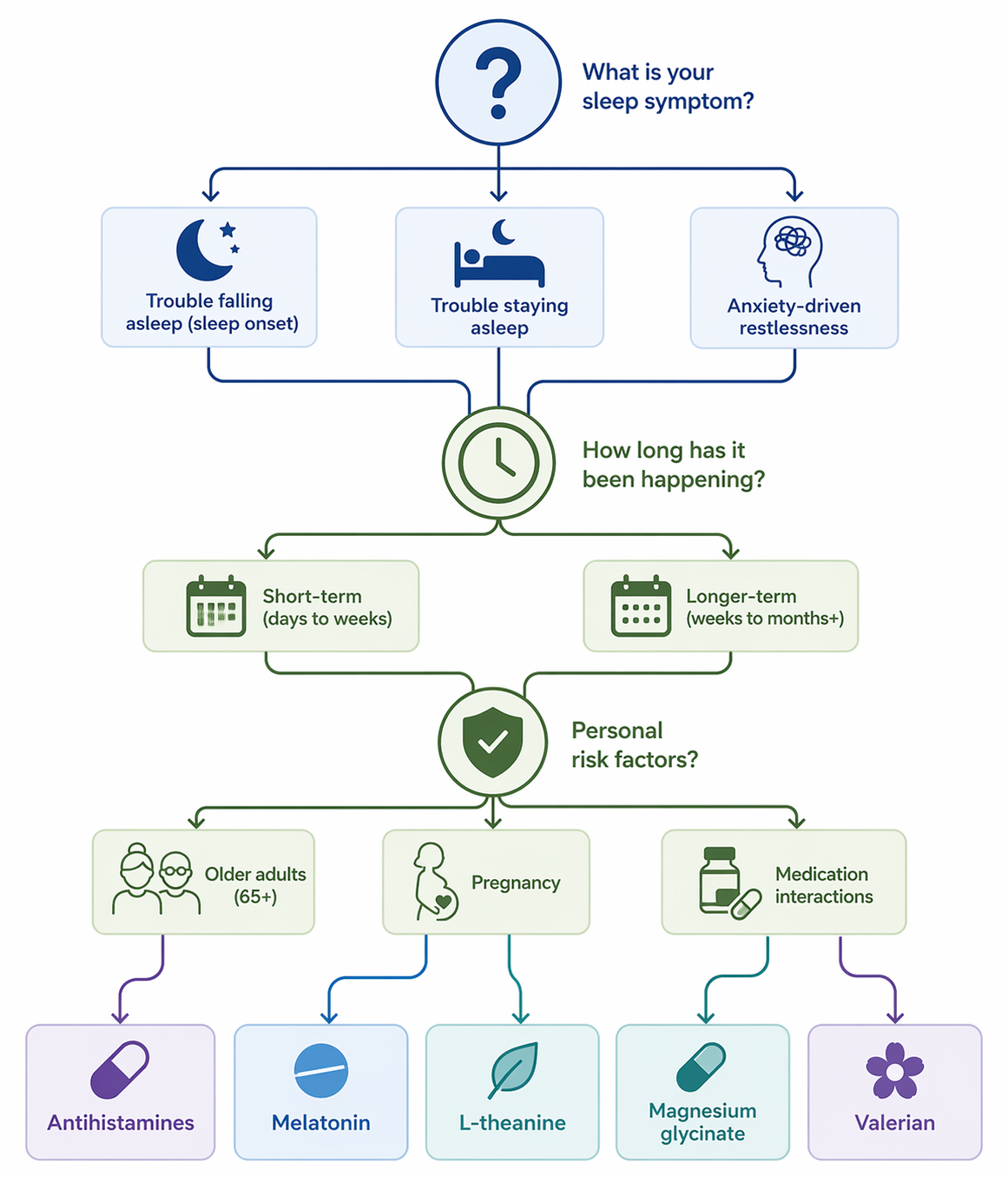
Before comparing labels, sort the problem. Most OTC sleep-aid confusion comes from using one blunt question — “What works?” — when you need three narrower ones.
- What is the main sleep problem: falling asleep, staying asleep, or feeling too keyed up to relax?
- How long has this been happening: a few nights, a few weeks, or longer?
- Do you have a reason to avoid certain ingredients: age over 65, pregnancy, glaucoma, prostate enlargement, urinary retention, other sedating medicines, alcohol use, or multiple prescriptions?
If you are not sure whether your main problem is sleep onset or sleep maintenance, pause there first. The difference changes the decision; a deeper symptom triage is covered in Trouble Falling Asleep vs. Staying Asleep.
| Your situation tonight | Ingredient category to consider | Why it may fit | When to pause |
|---|---|---|---|
| A few acute bad nights after travel, stress, grief, or schedule disruption | Diphenhydramine or doxylamine | More direct short-term sedation | Avoid casual nightly use; be especially cautious if over 65, pregnant, taking other sedatives, or prone to urinary retention |
| You feel sleepy too late, have trouble falling asleep, or suspect timing is off | Melatonin | Best used as a timing signal, usually at low doses | Choose third-party-tested products; more is not usually better |
| You are tense, ruminating, or physically restless rather than needing heavy sedation | L-theanine, magnesium glycinate, or possibly valerian | May support relaxation or modest sleep quality improvement | Expect gentler effects; check interactions and avoid assuming “natural” means risk-free |
| Symptoms have lasted more than 2–3 weeks, include loud snoring or gasping, or leave you fatigued despite enough time in bed | Clinical evaluation instead of another OTC experiment | The issue may not be a simple short-term sleep-aid problem | Do not keep escalating OTC sedatives to cover persistent symptoms |
When an Antihistamine Makes Sense — and When It Does Not
Diphenhydramine and doxylamine are the familiar drugstore sedatives hiding behind many “nighttime” labels. Diphenhydramine appears in products such as Benadryl, ZzzQuil, and many generic sleep aids. Doxylamine appears in Unisom SleepTabs and some generic sleep-aid products. These are not interchangeable just because both are antihistamines.
The practical difference starts with duration. Diphenhydramine has a reported half-life of about 3 to 9 hours, while doxylamine is closer to 10 hours and may last 12 to 15 hours in older adults.[2][3][4] That is why “I took it at midnight and felt useless the next morning” is not a mysterious reaction. It is a predictable consequence of taking a sedating medication that may still be active when the alarm goes off.
There is also a difference between being knocked out and getting better sleep. OTC antihistamine users may spend as little as 5% of sleep time in deep sleep, compared with 10% to 25% in healthy sleepers.[5] That does not mean no one should ever use them. It does mean that the morning-after question matters: did you sleep in a way that helped, or were you simply sedated?
The appeal is real. If you have had three miserable nights and need one night of relief, a sedating antihistamine can feel like the only option with enough force behind it. The trade-off is that regular use can lose effectiveness quickly as tolerance develops, and the anticholinergic effects — dry mouth, constipation, confusion, urinary problems, and next-day impairment — are not side details.[2][6]
For adults 65 and older, the answer changes more sharply. The 2023 AGS Beers Criteria lists first-generation antihistamines such as diphenhydramine and doxylamine as potentially inappropriate for older adults because of anticholinergic risks.[6] If this is your age group, do not treat a front-of-store sleep aid as benign just because it is sold without a prescription. The older-adult warning deserves its own read; see OTC Sleep Aids for Older Adults.
Diphenhydramine also needs a harder stop for people with certain conditions. Mayo Clinic advises avoiding diphenhydramine if you have closed-angle glaucoma, prostate enlargement, or urinary retention.[2] Add other sedating medicines, alcohol, or complex medication lists, and the safest choice may be no OTC sedative until a pharmacist or clinician reviews the full picture.
If your decision has narrowed to these two ingredients, use the ingredient name rather than the brand name. For a deeper head-to-head safety comparison, see doxylamine vs. diphenhydramine.
Melatonin Is Usually a Timing Tool, Not a Stronger Sedative
Melatonin is most useful when the problem is falling asleep at the right time: jet lag, a shifted schedule, or lying awake because your body does not seem ready for sleep yet. It is less convincing as a general-purpose answer for every form of insomnia.
Dose is where many shoppers go wrong. Common guidance from sleep-health sources puts the useful adult range around 0.5 to 3 mg, and doses above 5 mg rarely add benefit while increasing the chance of grogginess or vivid dreams.[7][8] A 10 mg gummy may look more serious. It is not automatically a better sleep aid.
The bigger problem is label trust. A 2023 JAMA analysis found that 88% of tested melatonin gummy products were inaccurately labeled; broader analyses have found more than 70% of melatonin supplements mislabeled.[9] That changes the buying advice. If you choose melatonin, look for third-party certification rather than assuming the dose on the front of the bottle is what you are getting.
Older adults often need even less melatonin than younger adults, but very low-dose products can be harder to find in U.S. stores. Liquids or tablets that can be split may make more sense than high-dose gummies. If you take blood thinners, seizure medicines, diabetes medicines, immune-suppressing drugs, or several prescriptions, ask before adding it.
If the Problem Is Restlessness, Consider Gentler Options With Modest Expectations
Some nights do not call for pharmacologic sedation. They call for turning down the physical and mental activation that keeps sleep from starting. That is where L-theanine, magnesium glycinate, and valerian enter the conversation — not as miracle substitutes, but as options that may better fit a relaxation-driven problem.
L-theanine is commonly discussed around 200 mg and is associated with relaxation and alpha-wave activity without acting like a classic sedative.[8] It may fit the person who says, “I am tired, but my body will not unclench.” For a closer look at dose and safety, see L-Theanine for Sleep.
Magnesium glycinate is usually chosen for tolerability, and clinical-trial evidence suggests modest sleep-quality benefits rather than dramatic sedation. One practical dose reference is about 127 mg elemental magnesium, not 127 mg of the total compound. That distinction matters because supplement labels can make the number look simpler than it is. For more detail, see magnesium glycinate for sleep.[8]
Valerian has a longer history as an herbal sleep aid, and the 2025 scoping review placed it with melatonin among the OTC options with the strongest evidence for effectiveness and safety.[1] That is still not the same as guaranteed benefit. Valerian products vary, and people taking sedatives or other medications should be cautious. A fuller evidence review is available in Does Valerian Root Actually Help You Sleep?.
If anxiety is clearly the main driver — racing thoughts, dread about sleep, a wired feeling at bedtime — the better decision may be to match the aid to the anxiety pattern rather than keep testing stronger sedatives. That narrower pathway is covered in The Best OTC Sleep Aid for Anxiety Depends on Your Primary Symptoms.
Pregnancy and Medication Lists Change the Shelf Decision
Pregnancy is not the time to freestyle with sleep-aid labels. Doxylamine combined with pyridoxine is FDA-approved for nausea and vomiting of pregnancy and has extensive post-1970s safety data, but that does not automatically turn every doxylamine sleep-aid use into a do-it-yourself pregnancy sleep plan.[3] The symptom, dose, timing, and your clinician’s guidance matter.
If you are pregnant or trying to become pregnant, use a pregnancy-specific safety source before buying. Start with Which Sleep Aids Are Safe During Pregnancy? and bring the actual bottle or ingredient list to your OB-GYN, midwife, or pharmacist.
Medication interactions deserve the same respect. The risk is not only one ingredient; it is the stack. A sedating antihistamine plus alcohol, a benzodiazepine, an opioid pain medicine, some antidepressants, muscle relaxers, or other nighttime products can turn a “simple” OTC choice into next-day impairment, falls, or breathing risk. If the label says “PM,” check whether it contains diphenhydramine or doxylamine before combining it with anything else.
How to Read the Label Without Getting Pulled Around by Branding
| What the package may say | Ingredient to look for | What that means for the decision |
|---|---|---|
| Benadryl, ZzzQuil, many “nighttime” generics | Diphenhydramine | Short-term sedating antihistamine; avoid with certain urinary, prostate, and glaucoma risks |
| Unisom SleepTabs, some store-brand sleep tablets | Doxylamine | Longer-lasting sedating antihistamine; higher next-day grogginess concern, especially in older adults |
| Melatonin gummies, tablets, liquids | Melatonin | Best for timing and sleep onset; choose low dose and third-party testing |
| Calm, relaxation, stress-support sleep supplements | Often magnesium, L-theanine, botanicals, or blends | May fit restlessness; effects are usually subtler and blends complicate interaction checks |
| Valerian root capsules, teas, tinctures | Valerian | Some supportive evidence, but product variability and interactions still matter |
Combination products are where responsible choices get harder. A product can contain melatonin plus herbs plus magnesium plus a sedating antihistamine, and the front label may still read like one gentle sleep formula. Turn the bottle around. The active ingredient and supplement facts panel matter more than the sleep promise on the front.
When the Best OTC Choice Is to Stop Shopping
OTC sleep aids are best suited to occasional, short-term problems. If insomnia has lasted beyond 2 to 3 weeks, if someone tells you that you snore loudly or gasp during sleep, or if you feel persistently fatigued despite giving yourself enough time in bed, the decision has moved beyond which bottle to buy.
At that point, another stronger sedative can delay the useful answer. Sleep apnea, restless legs, medication effects, mood disorders, pain, reflux, hormonal changes, and chronic insomnia patterns all need different approaches. For self-care triage before a clinical visit, see Insomnia Self-Care or the broader Insomnia FAQ.
For a few bad nights, choose proportionately: antihistamine only if short-term sedation is really what you need and you have screened for risk; melatonin if timing is the problem; L-theanine, magnesium glycinate, or valerian if relaxation support fits better. If the pattern is no longer occasional, do not keep asking the drugstore shelf to solve a medical question.
References
- Over-the-counter products for insomnia in adults: A scoping review of randomised controlled trials, Sleep Medicine, 2025.
- Sleep aids: Understand options sold without a prescription, Mayo Clinic.
- Doxylamine, StatPearls.
- Doxylamine vs. Diphenhydramine: Here Are the Differences, GoodRx.
- Over-the-Counter (OTC) Medications as Short-Term Sleep Aids, Spine-Health.
- Are drugstore sleep aids safe?, Harvard Health.
- Melatonin Dosage: How Much Melatonin Should I Take?, Sleep Foundation.
- Natural Sleep Aids: Which Are the Most Effective?, Sleep Foundation.
- What to Know About Over-the-Counter Sleep Aids, Cleveland Clinic.


Comments
Join the discussion with an anonymous comment.