If chronic pain has been waking you at 3 a.m., the usual sleep advice can start to sound almost insulting. Make the room dark. Stop scrolling. Cut caffeine. Keep a schedule. Those steps may help at the edges, and for some people they are enough. But a hip that throbs when you roll over, a lower back that stiffens after four hours in bed, jaw pain that surges before dawn, or nerve pain that burns through a quiet room is not simply a bedtime-behavior problem.
The more useful starting point is this: chronic pain and sleep quality feed each other through the nervous system. Pain fragments sleep. Fragmented sleep lowers pain tolerance. The next day begins with a body that is less restored and a pain-signaling system that is easier to provoke. By the next night, the pain is louder, the bed is less neutral, and sleep has more to fight through.

That loop is common enough that it should not be treated as a rare complication. A 2022 review by Whale and Gooberman-Hill reported that an estimated 67% to 88% of people with chronic pain experience sleep disruption, while at least half of people with insomnia report chronic pain.[1] The overlap is not just a matter of discomfort making sleep inconvenient. It is one of the places where pain care and insomnia care need to meet.
The Loop Does Not Run Equally in Both Directions
It is easy to say pain and sleep affect each other. The more clinically useful question is whether one side of the loop often moves first. The evidence is not perfectly uniform across every pain condition, but the pattern is important: sleep impairment often predicts next-day pain more strongly than pain predicts next-night sleep.[1]
That does not mean pain is imaginary, or that poor sleep is the sole cause of chronic pain. It means sleep is not merely the victim of pain. A bad night can change the sensitivity of the system that will interpret signals the next day. For someone with arthritis, fibromyalgia, neuropathy, migraine, temporomandibular pain, inflammatory disease, or persistent back pain, that distinction matters. Treating insomnia is not cosmetic self-care layered on top of “real” pain treatment. It can be one of the places where pain amplification is addressed.
The Sleep Foundation’s overview of pain and sleep describes the relationship in similar bidirectional terms: pain can make it harder to fall asleep and stay asleep, while poor sleep can heighten sensitivity to pain and worsen pain-related distress.[2] That broad framing is useful, but chronic pain patients usually need more than a broad framing. They need to know why the body can feel punished after one short, broken night.
What Sleep Loss May Be Doing to Pain Signaling
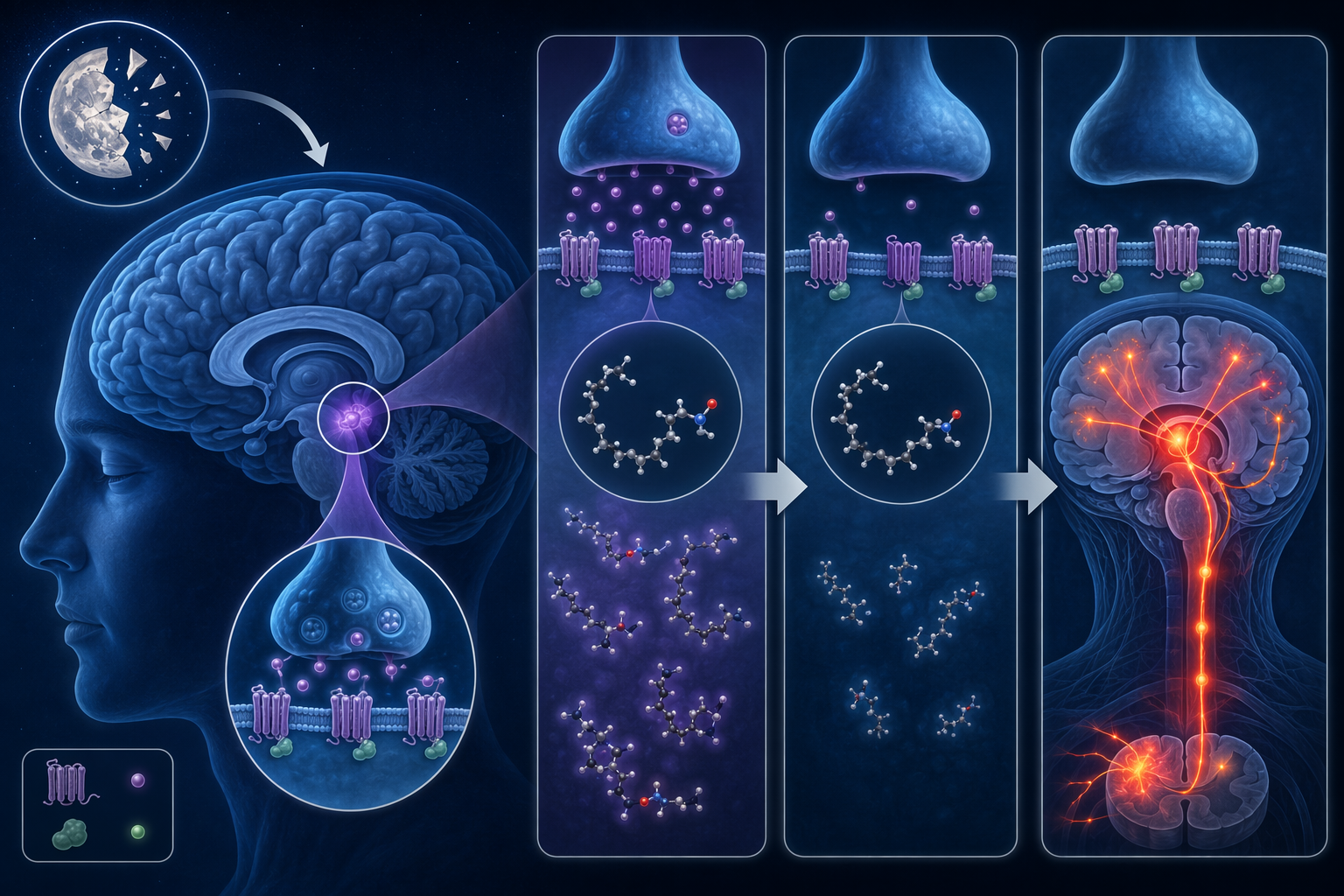
One of the most interesting recent clues comes from a 2023 Harvard Medical School and Massachusetts General Hospital study discussed by the Harvard Gazette. In a mouse model, researchers found that sleep deprivation reduced levels of N-arachidonoyl dopamine, or NADA, an endocannabinoid in the brain. NADA normally helps dampen pain signaling through cannabinoid receptor 1, known as CB1. When sleep deprivation depleted NADA, pain sensitivity increased; when the researchers restored NADA in a relevant brain region, pain sensitivity was reduced.[3]
The boundary belongs right next to the finding: this was mouse research, not proof that the same mechanism explains every human pain flare after poor sleep. It is better read as a leading biological hypothesis under investigation than as a finished clinical rule. Still, it gives the pain-sleep loop a molecular hinge. Sleep loss may not simply make people crankier, less resilient, or more aware of symptoms. It may reduce one of the brain’s own pain-dampening signals.
That matters because it changes the moral tone of the problem. A person who hurts more after a bad night is not necessarily catastrophizing, failing at relaxation, or paying too much attention to symptoms. The nervous system may be operating with weaker inhibition. Pain messages that might have been filtered more effectively after consolidated sleep can arrive with less braking.
Deep Sleep, Pain Modulation, and Inflammation
NADA is not the whole story. Chronic pain also disrupts sleep architecture, especially the deeper stages of sleep that are often discussed as slow-wave sleep. When pain repeatedly pulls the brain toward lighter sleep or wakefulness, the night may look adequate on the clock while still being physiologically poor. Eight hours in bed is not the same as eight hours of restorative sleep.
Slow-wave sleep disruption has been associated with increased pain sensitivity and reduced conditioned pain modulation, the body’s ability to dampen one painful input when another competing input is present.[1] Put less technically, the system that should help turn pain volume down may not work as well after disrupted sleep. This is one reason “I slept, but I woke up hurting everywhere” can be a real description rather than an exaggeration.
Inflammation adds another bridge between the two sides of the loop. A 2016 systematic review and meta-analysis by Irwin and colleagues found that sleep disturbance and long sleep duration were associated with increases in markers of systemic inflammation, and experimental sleep deprivation was also linked with inflammatory changes.[4] Inflammation is not the explanation for every chronic pain condition, and inflammatory markers are not bedside instructions. But the finding helps explain why sleep disruption can have consequences beyond next-day fatigue.
These mechanisms can stack. Pain interrupts sleep. Interrupted sleep reduces deep-sleep continuity, weakens pain modulation, may alter inflammatory activity, and, according to the mouse-model NADA work, may reduce endocannabinoid pain-dampening. The next day’s pain is then being interpreted by a system that has had less recovery and less inhibition. That is the loop readers recognize in their bodies, described with more precision.
Sleep Problems May Come Before Widespread Pain
The relationship also appears to matter before chronic widespread pain is established. A Swedish prospective population study followed people who were pain-free at baseline and found that sleep problems predicted the later onset of chronic widespread pain over 5-year and 18-year follow-up periods.[5] That does not prove that insomnia alone causes widespread pain. Prospective studies can strengthen the timeline, but they do not erase every other biological, psychological, occupational, and medical factor.
Still, the direction is hard to ignore. If poor sleep can precede later widespread pain in some people, sleep deserves attention before pain has expanded, not only after years of symptoms have made the pattern obvious. It also supports a more protective approach to persistent insomnia in people who already have localized pain. Waiting until the pain condition becomes more entrenched is not a neutral choice.
Why Sleep Hygiene Alone Often Lacks Enough Force
Basic sleep hygiene still has a place. A regular wake time, morning light, a cooler room, less evening alcohol, and a realistic caffeine cutoff can remove avoidable barriers to sleep. If a person has never been taught the fundamentals, a simple baseline such as sleep hygiene fundamentals and an evidence-based bedtime routine is a reasonable starting point.
But sleep hygiene is usually too passive for the chronic pain loop. It mainly adjusts the environment and daily habits around sleep. It does not directly retrain the bed-pain-wakefulness association, reduce time spent awake in bed, restructure fear about sleeplessness, or consolidate sleep after months or years of fragmented nights. Those are different clinical tasks.
This is the same reason generic advice often fails specific groups: the advice may be sound in general, but too blunt for the mechanism in front of it. Older adults with sleep disruption, for example, often need more than standard hygiene reminders because medical conditions, medications, circadian changes, and nighttime awakenings complicate the picture, a limitation discussed in why sleep hygiene advice often fails older adults. The same logic applies here: the pain-sleep loop is not fixed by pretending it is an ordinary bedtime-routine problem.
Pain Medication Can Help Pain and Still Disturb Sleep
There is another clinical wrinkle worth naming carefully. Better pain control can improve sleep for many people, and untreated pain should not be romanticized as something to breathe through indefinitely. But some pain medications can also affect sleep architecture. Cleveland Clinic pain specialist Dr. Robert Bolash has noted that opioid pain medications can disrupt sleep architecture, including the stages of sleep that help people feel restored.[6]
That does not mean a person should stop prescribed medication because an article mentioned sleep architecture. It means the pain-sleep conversation belongs with a clinician who can review the whole picture: pain diagnosis, medication timing, dose, breathing risk, other sedating drugs, mood symptoms, sleep apnea risk, and whether insomnia has become its own treatable condition. Pain treatment and sleep treatment should be coordinated, not assumed to be the same thing.
The Treatment Implication: Treat Insomnia Directly
Once sleep is understood as an active regulator of pain sensitivity, the treatment hierarchy becomes clearer. The first serious question is not which pillow, supplement, mattress, wearable, or sound machine might soothe the night. The question is whether insomnia has become a maintained disorder that needs insomnia treatment.
Cognitive behavioral therapy for insomnia, or CBT-I, is the main evidence-based treatment to know. It is not generic “think positive” therapy. CBT-I uses structured methods such as stimulus control, sleep restriction or sleep consolidation, cognitive work around sleep-related fear, and behavioral scheduling to rebuild sleep drive and reduce conditioned wakefulness in bed. Cleveland Clinic describes CBT-I as effective for many patients and reports that 70% to 80% of patients with pain respond to the treatment in clinical practice.[6]

That figure should be encouraging, not inflated into a guarantee. Clinical-practice response rates can look stronger than the more modest average effects reported in some meta-analyses, and people with chronic pain vary widely by diagnosis, medication use, mental health burden, disability level, and access to care.[1][6] Still, CBT-I is important because it aims at the mechanism maintaining insomnia, not merely the bedroom conditions surrounding it.
For a chronic pain patient, CBT-I may involve uncomfortable but purposeful changes. Spending less time awake in bed can initially mean a tighter sleep window. Getting out of bed when unable to sleep can feel unrealistic when movement hurts, so the plan may need adaptation. Cognitive work may focus less on generic worry and more on pain-specific predictions: “If I do not sleep tonight, tomorrow will be unbearable,” or “The bed is where pain takes over.” A good CBT-I plan respects the pain condition while still treating the insomnia pattern.
The site’s deeper explainer, What Actually Cures Insomnia? CBT-I Explained, is the natural next step if insomnia has lasted for weeks or months, especially when bed has become a place of pain monitoring, frustration, and alertness.
What to Do With This Information
The practical move is not to turn every bad night into a neuroscience project. It is to stop treating chronic pain and sleep quality as separate problems when they are clearly reinforcing each other. If pain repeatedly wakes you, if you spend long stretches awake in bed because pain has made the bed feel unsafe, or if every short night reliably produces a higher-pain day, insomnia deserves direct clinical attention.
A useful treatment hierarchy looks like this: keep the basic sleep hygiene steps that remove obvious friction; work with a clinician on the pain condition and medication context; screen for sleep disorders such as sleep apnea when symptoms or risk factors point that way; and consider CBT-I when insomnia has become persistent. In chronic pain, sleep is not just recovery time stolen by symptoms. It is one of the active regulators of pain sensitivity, and treating insomnia directly can be part of pain care.
References
- The importance of sleep for people with chronic pain: current insights and evidence, Whale K, Gooberman-Hill R., 2022.
- Pain and Sleep, Sleep Foundation.
- Sleep deprivation enhances pain sensitivity via the endocannabinoid system, Harvard Gazette, 2023.
- Sleep Disturbance, Sleep Duration, and Inflammation: A Systematic Review and Meta-Analysis of Cohort Studies and Experimental Sleep Deprivation, Biological Psychiatry, 2016.
- Sleep problems and chronic widespread pain: a population-based longitudinal study, Swedish prospective population study.
- Managing Chronic Pain and Insomnia, Cleveland Clinic.






Comments
Join the discussion with an anonymous comment.