The unsettling part of wildfire smoke sleep disruption is that it can continue after the visible danger has eased. The air quality app may look less alarming. The evacuation order may be lifted. The cough may be fading. Yet the body still treats bedtime as a surveillance shift: listening for sirens, checking the window glow, noticing every throat tickle, waking from dreams with the feeling that something is already wrong.
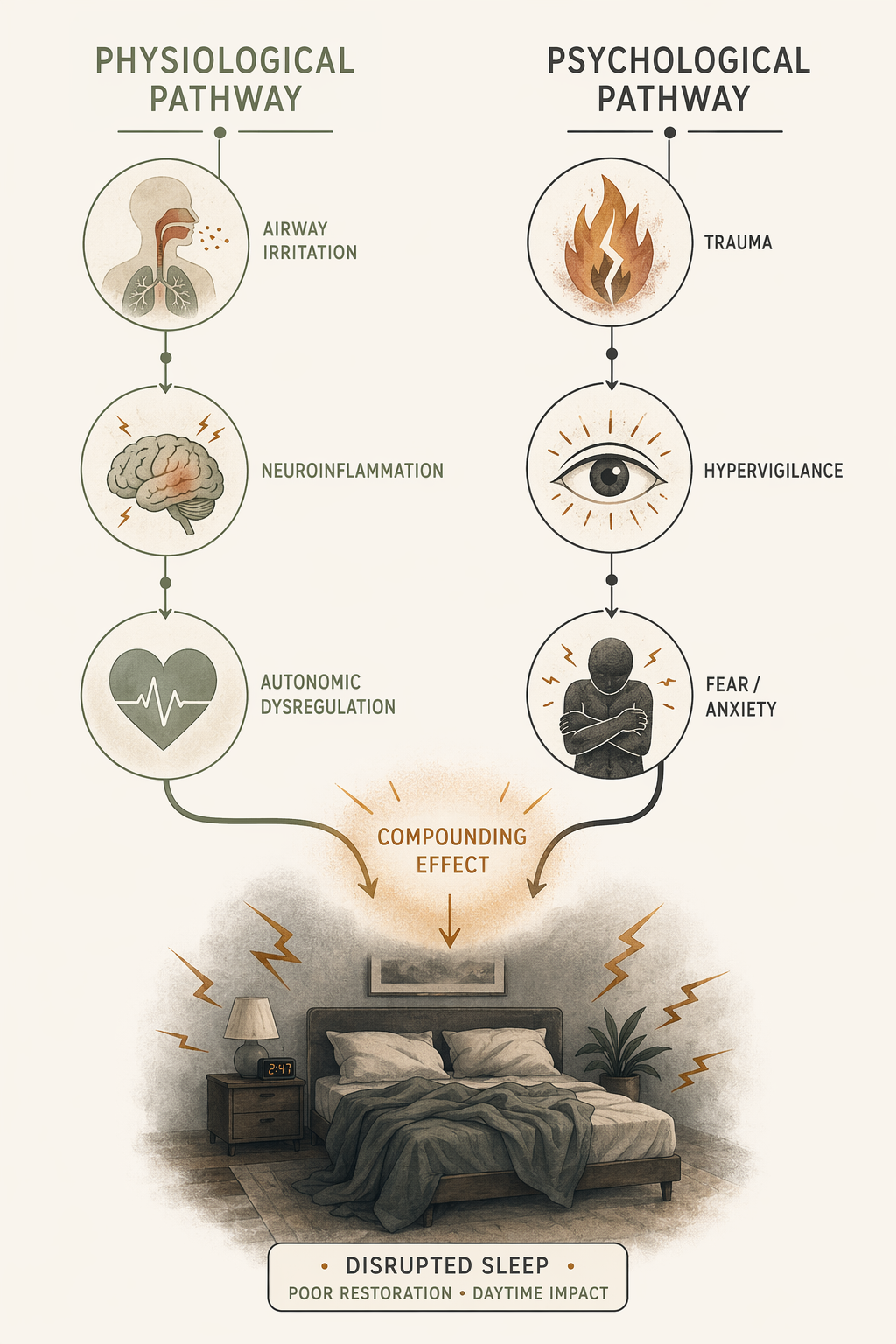
That mismatch is not imaginary. Wildfire smoke can disturb sleep through a direct physical route and through a threat-response route, and the two often feed each other. Smoke irritates the airway, can contribute to inflammatory stress, and can keep the autonomic nervous system more activated than sleep comfortably allows. At the same time, the experience of fire, evacuation, uncertainty, property loss, or repeated smoke alerts can train the brain to treat night as a vulnerable time. The bed becomes less a recovery space than a place where the next warning might arrive.

The prevalence numbers are rough, but they are hard to dismiss. A 2021 systematic review found insomnia in 63% to 72.5% of wildfire survivors measured one to ten months after a fire, and nightmares in 33.3% to 46.5%; the authors noted that these insomnia rates were roughly double a general population estimate of about 30%.[1] That does not mean every person who sleeps badly after smoke exposure is developing a disorder. The same review found only five eligible studies, and the studies were too different for a meta-analysis.[1] It does mean that persistent post-fire sleeplessness is common enough to deserve more than a shrug.
Smoke can wake the body before fear enters the room
The physical route is the easier one to recognize. Fine particulate matter in wildfire smoke can irritate the nose, throat, and lower airway. A person may fall asleep and then wake coughing, congested, dry-mouthed, or short of breath. Even milder irritation can fragment sleep because the sleeping brain still monitors breathing. If each breath feels slightly effortful, sleep becomes lighter.
This is why a smoke night can feel different from an ordinary bad night. The discomfort is not only environmental; it becomes bodily evidence. A tight chest may be from irritation, asthma, anxiety, or all of them at once. Once the brain has paired that sensation with danger, the sensation itself can become an alarm. The distinction between physical and psychological pathways is useful for thinking, but it is not clean in lived experience.
For a broader companion explanation of the physical and psychological routes, see How Wildfires Affect Sleep Quality Through Two Pathways. Here, the sharper question is what happens when the smoke improves but sleep does not.
The psychological pathway can outlast the air quality alert
During an active smoke event, bad sleep is expected. Windows are closed. Rooms are warmer. Alerts arrive late. People check maps, message family, and decide whether to leave. Sleep may be shortened because there is too much to monitor.
Afterward, the pattern should gradually loosen. The person may still sleep lightly for several nights, but the nervous system begins to accept new information: the air is safer, the fire is contained, the immediate decisions are over. When that recalibration does not happen, sleep starts to carry the threat forward. The person may delay bedtime because lying down feels unsafe. They may wake with a surge of adrenaline and scan for smoke. They may have nightmares that do not replay the fire exactly but carry the same physics: trapped, separated, unable to breathe, unable to get out.
That is where wildfire smoke sleep disruption becomes clinically more important than ordinary short-term restlessness. Sleep is no longer only being interrupted by conditions outside the body. Sleep itself has become associated with danger.
Insomnia and nightmares can be early warning signs after wildfire exposure
The strongest reason not to minimize persistent post-fire sleep symptoms is their relationship with PTSD. In a study conducted one month after wildfire exposure, insomnia was present in 79.1% of people diagnosed with PTSD. Nightmares were also much more common among those with PTSD than among those without it: 46.5% versus 12.3%.[2]
The timing matters. One month post-fire is not the same as a long-term follow-up, and it cannot tell every person’s future trajectory. But it does show that insomnia and nightmares are not incidental details in the aftermath. They sit close to the fear system, and in some survivors they may mark a trauma response that is still consolidating.
This is also why treating sleep as merely a secondary PTSD symptom can be too passive. If a person is sleeping poorly because bedtime triggers fear, then waiting for every other trauma symptom to resolve before addressing sleep may leave one of the reinforcing loops untouched. Broader sleep-trauma research supports early sleep intervention as a possible PTSD prevention target, although wildfire-specific randomized prevention trials have not yet established that effect in exposed populations.[1]
The useful framing is bidirectional. Trauma can disturb sleep, and disturbed sleep can make fear learning, emotional regulation, and daytime coping harder. That same bidirectional logic appears in other sleep and mood conditions; for a related explanation, see How depression and insomnia fuel each other.
When bad sleep is still an acute stress response
It is possible to take post-wildfire sleep seriously without turning every bad night into a diagnosis. During active smoke, evacuation, displacement, heat, school closure, work disruption, or insurance uncertainty, sleep may be poor because life is genuinely unstable. A nervous system that stays alert during an unresolved threat is doing something understandable.
Acute disruption usually tracks the conditions around it. Sleep worsens when smoke thickens, when alerts increase, when the room is hot, when coughing is worse, or when a person has to make safety decisions. As those pressures ease, sleep may remain imperfect but begins moving in the right direction. The person may still wake earlier than usual, but they can return to sleep. They may feel tense at bedtime, but they do not organize the evening around avoiding sleep.
| Pattern | More consistent with short-term disruption | More concerning for emerging insomnia |
|---|---|---|
| Timing | Sleep worsens mainly during active smoke, evacuation, or immediate instability | Sleep remains poor after air quality and immediate danger improve |
| Bedtime response | Tension fades as routines and safety return | Bedtime itself starts to feel threatening or unsafe |
| Awakenings | Waking is tied to coughing, alerts, heat, or noise | Waking comes with panic, scanning, dread, or repeated fear-based arousal |
| Dreams | Bad dreams are occasional and decrease over time | Nightmares are recurrent, distressing, or lead to avoiding sleep |
| Daytime effect | Fatigue improves as sleep opportunity improves | Poor sleep causes ongoing impairment, mood strain, concentration problems, or fear of the next night |
The dividing line is not one perfect number of nights. It is the direction of recovery. If safety cues are returning but the sleep system is not updating, the problem deserves attention.
How sleep becomes something to avoid
A common sequence is quiet and gradual. First, smoke makes sleep physically unpleasant. Then the person starts watching the evening conditions: wind direction, AQI, alerts, smell in the hallway. Then they begin sleeping lightly because they do not fully trust the night. After a few frightening awakenings or nightmares, the bed becomes associated with the moment danger returns.
Avoidance can look sensible from the inside. Staying up feels safer than lying down. Sleeping on the couch near the door feels safer than the bedroom. Keeping the phone bright and close feels safer than letting the night go quiet. These strategies may help someone get through the first days of a crisis, but they can later teach the brain that sleep requires guarding.
Nightmares intensify the loop because they make sleep feel like exposure to the threat rather than relief from it. A person may begin to fear the dream before it happens. Once that fear enters the evening, insomnia can become self-sustaining even if the original smoke exposure has lessened.
Smoke is also a mental health exposure
The sleep story fits a wider mental health pattern. A 2025 JAMA Network Open study reported that a 10 μg/m³ increase in wildfire-specific PM2.5 was associated with increased emergency department visits for depression, anxiety, and mood disorders up to seven days after exposure.[3] The finding matters because it pushes back against the narrow idea that smoke is only a respiratory event.
It also needs its limits. The study examined California’s 2020 wildfire season, described by the Harvard T.H. Chan School of Public Health as the most severe on record, and the results may not generalize neatly to lower-severity seasons or other regions.[3] Still, for people who felt emotionally worse during smoke days, the association is clinically recognizable: the same exposure that burns the throat can also increase anxiety, mood instability, and vigilance.
Risk is not evenly distributed. The Harvard report identified women, children and young adults, Black and Hispanic individuals, and Medicaid enrollees as groups with the highest risk for smoke-linked mental health emergency visits in that California analysis.[3] Sleep-focused wildfire research also points to greater vulnerability among women, older adults, and people with prior trauma histories.[1] These patterns should not be used to predict an individual’s outcome with false certainty, but they do help explain why two people in the same smoke event may recover very differently.
Children may show the pattern before they can explain it
Children deserve separate mention because sleep may be one of the clearest ways distress appears. In one high-loss wildfire scenario cited in the Isaac review, children had insomnia rates of 69.2% at six weeks and 84.6% at ten weeks after the fire.[1] The sample and context should not be stretched into a universal forecast, but the direction is sobering: sleep problems can worsen over the early aftermath rather than simply fade once the flames are out.
A child may not say, “I am hypervigilant.” They may ask to sleep with a parent, resist bedtime, complain of stomachaches, wake from dreams, or become irritable in the evening. For families, the question is not whether the child is being dramatic. It is whether sleep is gradually regaining safety or becoming the place where the disaster keeps replaying.
When to treat the sleep problem directly
The clearest reason to seek help is not that the sleep problem began during a wildfire. It is that sleep is no longer recovering with safety. Clinical attention is especially warranted when insomnia persists after air quality improves, when nightmares are recurrent or lead to sleep avoidance, when panic-like awakenings continue, when daytime functioning is impaired, or when the person feels trapped in monitoring behaviors that no longer match the actual conditions.
Care should match the mechanism. If airway symptoms, asthma, chest pain, or breathing problems are part of the night, medical evaluation matters. If fear, trauma reminders, or sleep avoidance are driving the pattern, the sleep treatment should not pretend this is ordinary poor sleep hygiene. CBT-I can help reduce the behaviors and expectations that keep insomnia going, and trauma-adapted sleep care may be needed when nightmares and hyperarousal are central. For a practical starting point on anxiety-driven sleeplessness, see What to Do When Anxiety Keeps You Up at Night.
Air purifiers, masks, sealed bedrooms, and cleaner indoor air can be important during smoke exposure, but they do not fully answer the post-event sleep question. A safer room can reduce physical triggers. It cannot, by itself, teach a threatened nervous system that sleep is safe again.
The practical distinction is therefore narrower and more useful than asking whether the reaction is “normal.” During and soon after a wildfire or smoke episode, disrupted sleep may be an expected stress response. But if the air clears and the brain keeps assigning danger to bedtime, the sleep problem has become part of the threat system. That is the point where insomnia and nightmares deserve care in their own right.
References
- A Systematic Review of the Impact of Wildfires on Sleep Disturbances, International Journal of Environmental Research and Public Health, 2021.
- Insomnia and PTSD one month after wildfires: Evidence for an independent role of the fear of imminent death, PubMed, 2017.
- Exposure to wildfire smoke linked with worsening mental health conditions, Harvard T.H. Chan School of Public Health, April 2025.






Comments
Join the discussion with an anonymous comment.