Yes: wildfire smoke can affect sleep quality, and the most useful explanation is not simply that smoke is unpleasant or anxiety-provoking. The stronger physiological case is that smoke can interfere with the architecture of sleep itself: the cycling through non-rapid eye movement sleep, rapid eye movement sleep, and brief periods of wakefulness that determine whether a night is restorative.
The clearest experimental signal so far comes from a 2025 EPA-funded rodent study by Rentschler and colleagues. After a single 1-hour exposure to wildfire-relevant smoke, rats showed reduced NREM sleep duration, reduced REM sleep duration, and increased wakefulness during the rest period, measured with EEG rather than inferred from behavior. The same study linked those sleep-architecture changes with autonomic effects and concurrent blood pressure increases, which matters because sleep is not just a conscious state; it is a regulated cardiovascular and neurological state.[1]

That does not mean a 1-hour exposure in rats can be read as a precise prediction for every adult lying in a sealed bedroom during a smoke advisory. It does mean the question has moved beyond “smoke makes people uncomfortable.” The body has several routes by which inhaled wildfire particles can plausibly turn an 8-hour night into a lighter, more fragmented one.
Those routes tend to stack: irritated airways disturb breathing, fine particles shift autonomic regulation toward higher alert, and some particle-related inflammatory effects may reach sleep-regulating brain systems. The relative contribution of each pathway will differ by exposure level, filtration, baseline respiratory health, cardiovascular vulnerability, and whether the person is also dealing with evacuation, loss, or acute fear.
Smoke Does Not Have to Wake You Fully to Damage the Night
A sleeper does not need to bolt upright coughing for smoke to matter. Sleep can be degraded by events too small to remember in the morning: a brief rise in breathing effort, a swallow against throat irritation, a cough that barely reaches consciousness, or a shift out of deeper sleep into lighter sleep. These micro-arousals are one reason people can report “I slept all night” and still wake feeling as if the night never became solid.
Wildfire smoke is a mixture, but PM2.5 deserves special attention because particles in this size range can travel deep into the respiratory tract. In the upper airway, smoke can provoke throat irritation, nasal congestion, and postnasal drip. In the lower airway, it can increase airway resistance and make each breath slightly more effortful. During sleep, when muscle tone changes and ventilatory control is already more vulnerable, that extra resistance can be enough to fragment sleep continuity.
This is the part many generic sleep tips miss. Closing windows can reduce exposure, but it does not make indoor air biologically irrelevant. Smoke particles can enter through leaks, doors, ventilation systems, and repeated entry into the home. A person may be indoors, far from the flames, and still breathing enough fine particulate matter to experience airway irritation during the hours when sleep is supposed to be most protected.
The connection to sleep-disordered breathing is suggestive rather than definitive. In a large study of air pollution and sleep apnea, higher annual exposure to PM2.5 and nitrogen dioxide was associated with greater odds of sleep apnea.[2] That does not prove that a smoke episode causes sleep apnea. It does make the airway pathway harder to dismiss, especially for people with borderline or undiagnosed obstructive sleep apnea, chronic rhinitis, asthma, COPD, or a tendency toward snoring when congested.
The Autonomic Pathway Is Where the Sleep Story Gets Sharper
Normal sleep is not passive shutdown. Across a healthy night, the autonomic nervous system changes its balance: parasympathetic activity generally becomes more prominent, heart rate and blood pressure tend to fall, and the body becomes more capable of sustaining deep NREM sleep and cycling into REM. That physiology is not decorative. It is part of what sleep is.
Fine particulate exposure pushes in the opposite direction. When PM2.5 reaches the lungs, it can trigger local inflammation and systemic signaling that affects vascular tone, heart rhythm regulation, and sympathetic nervous system activity. Heart rate variability is one way researchers track that shift. Lower or altered HRV patterns can indicate that the body is spending less time in the flexible, parasympathetic-dominant state that supports stable sleep.
This is why the 2025 Rentschler study is more important than a simple “animals slept less after smoke” headline. The study connected controlled smoke exposure with EEG-confirmed changes in sleep stages and physiological changes in autonomic and blood pressure regulation. Reduced NREM, reduced REM, and increased wakefulness appeared in the same experimental frame as cardiovascular activation, giving the mechanism a measurable bridge between inhaled smoke and altered sleep architecture.[1]
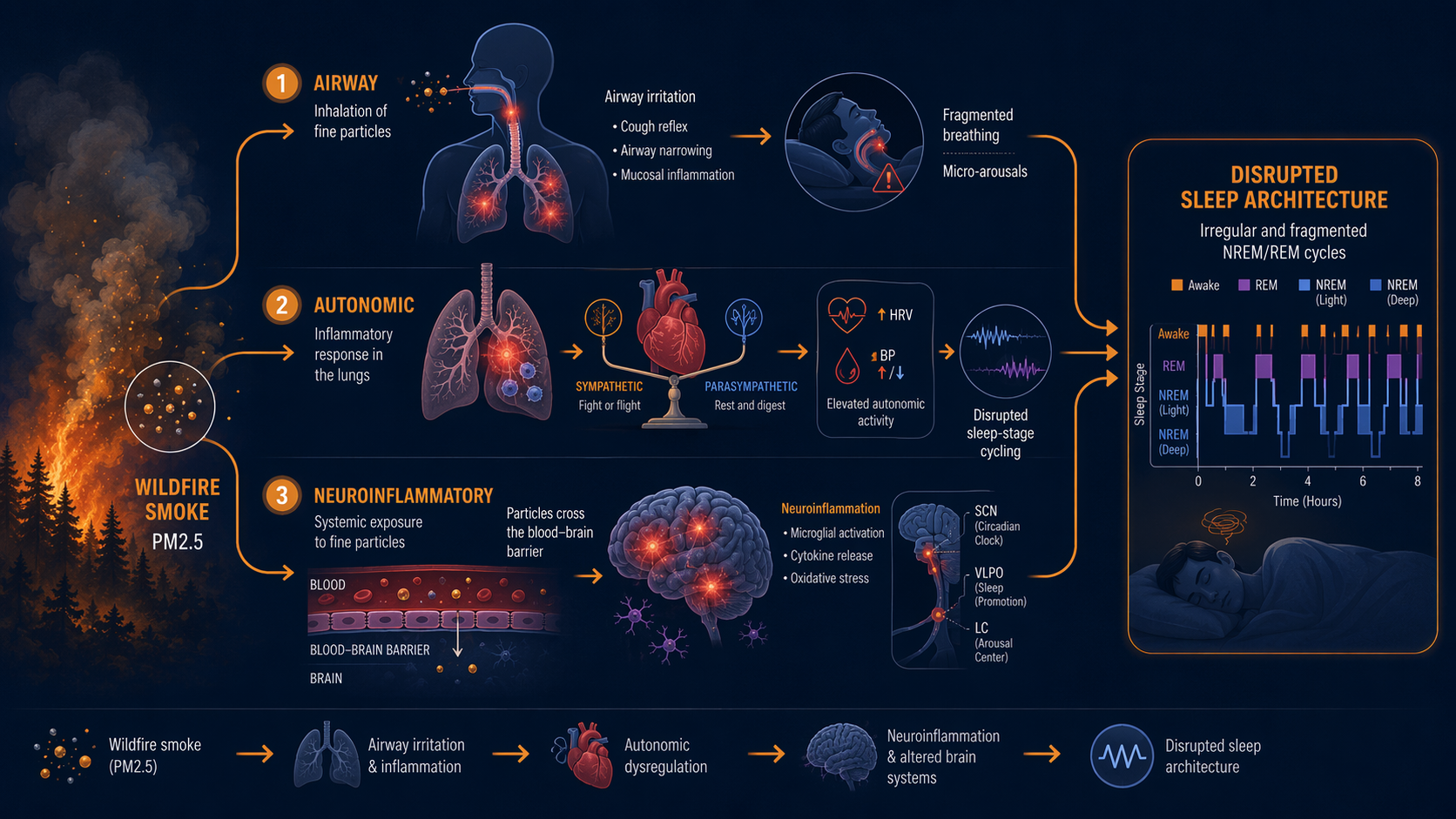
A higher-alert autonomic state is poorly matched to consolidated sleep. It can make sleep lighter, increase the probability of brief awakenings, and disturb the timing of transitions into deeper NREM and REM. REM sleep is especially dependent on coordinated autonomic and brain-state regulation; it is not surprising that a physiological stressor affecting cardiovascular control would show up there.
This also helps explain why people may feel a smoke-night hangover without remembering dramatic symptoms. The night may contain more wakefulness, more light sleep, or less sustained REM and NREM, but the sleeper’s memory system does not keep a clean log of every disturbance. The consequence is often recognized only after the fact: heavier morning fatigue, poorer concentration, a sense that the night was oddly shallow.
Airway Irritation and Sympathetic Activation Can Reinforce Each Other
The airway and autonomic pathways are often described separately because it makes the biology easier to follow. In a real bedroom, they are unlikely to stay separate. A congested nose increases mouth breathing. Mouth breathing can dry the throat and provoke coughing. Coughing and airway narrowing can raise arousal pressure. Repeated arousals then feed sympathetic activation, and sympathetic activation makes the body less able to settle into stable sleep.
For someone with sleep apnea risk, this stacking may matter more than the average exposure-response curve. Smoke-related congestion or airway inflammation does not need to create apnea from nothing to worsen a vulnerable night. It may increase respiratory effort, lengthen partial obstructions, or make recovery from a breathing disturbance more activating. The existing air-pollution and sleep-apnea association is therefore best used as a warning about susceptibility, not as proof of a single-cause relationship.[2]
A useful way to read the symptoms is by asking what changed. A dry, burning throat points toward irritation. New congestion or snoring points toward upper-airway narrowing. Palpitations, restless wake-ups, or a wired feeling in the middle of the night point more toward autonomic activation. None of these signs is specific to wildfire smoke, but during a smoke event they fit the physiology better than the idea that the problem is only worry.
The Brain Pathway Is Plausible, but Less Settled
The third pathway is the most tempting to overstate. Fine particles can penetrate deep into the lungs, enter circulation, and may influence the central nervous system through inflammatory signaling, vascular effects, or passage across protective barriers. Brain regions that regulate sleep and wakefulness are sensitive to inflammatory and immune signals, so the mechanism is biologically plausible.
But the evidence base is not equally strong across pollution sources. Neuroinflammatory effects are better established in research on traffic-related air pollution than in wildfire-smoke-specific human sleep studies. Wildfire smoke has a different chemical profile, and smoke episodes are often intermittent, intense, and mixed with heat, stress, evacuation risk, and changing indoor conditions. Those differences matter.
Non-human primate research adds plausibility without closing the case. California Air Resources Board-funded work reported that monkeys exposed to wildfire smoke PM2.5 showed reduced sleep duration and increased activity levels.[3] That finding is important because it moves beyond rodents and aligns with the idea that smoke can alter rest-activity patterns across species. It still does not replace EEG-confirmed sleep-stage measurement in humans, and it does not tell us how much of a typical adult’s smoke-season insomnia is driven by central nervous system inflammation rather than breathing disruption, autonomic activation, or stress.
Why Stress Alone Is an Incomplete Explanation
Wildfires are psychologically potent events. For people near an active fire, sleep disruption may come from evacuation alerts, fear, financial loss, trauma, displacement, and grief. Studies of wildfire survivors often capture that combined reality, and it would be artificial to pretend the mind and body separate cleanly during a disaster.
The narrower question here is different: can smoke itself disturb sleep in someone who is not in immediate danger? The mechanistic evidence says yes, plausibly. Airway irritation, altered HRV, blood pressure shifts, and EEG-measured changes in sleep stages do not require a person to be consciously afraid. Stress can amplify the disruption, but it is not needed to make the biology coherent.
That distinction is not academic. If a person assumes the whole problem is anxiety, they may try only relaxation strategies while ignoring exposure reduction, filtration, asthma control, apnea risk, or cardiovascular symptoms. Relaxation may still help the arousal component, and evidence on practices such as meditation for insomnia has a place, but smoke-season sleep disruption should not be reduced to a mindset problem.
The Cardiovascular Aftermath May Outlast the Bad Night
Sleep disruption and smoke exposure are not merely parallel burdens. They can interact. In a 2023 rodent study, sleep-disrupted rats exposed to eucalyptus smoke showed exaggerated morning blood pressure surges, increased cardiac output, and altered expression of genes regulating vasoconstriction.[4] The study was not a consumer sleep trial, and it should not be translated into a direct clinical forecast for one smoky night. It does show why researchers pay attention when smoke, sleep fragmentation, and cardiovascular regulation appear in the same chain.
Morning is already a physiologically active period. Blood pressure rises, cortisol rhythms shift, and the body moves from sleep into upright activity. If smoke exposure and fragmented sleep both push the cardiovascular system toward higher load, the transition out of sleep may become less benign for vulnerable people. That is especially relevant for adults with hypertension, arrhythmias, coronary disease, pregnancy-related risk, or chronic lung disease.
Why This Question Is Becoming Less Seasonal and Less Local
The scale of exposure has changed enough that smoke-related sleep disruption is no longer a niche concern for people living next to burning landscapes. Climate Central reported that per-person wildfire smoke exposure in the United States was 4 times higher in 2020–2024 than in 2006–2019.[5] That figure does not measure sleep quality, but it explains why more people are encountering the relevant exposure conditions indoors, overnight, and far from the fire perimeter.
Wildfire smoke also arrives during other environmental pressures on sleep. Hot nights can reduce the body’s ability to lose heat, and smoke events can coincide with closed windows, reduced ventilation, and anxiety about outdoor conditions. In the larger frame of climate change and sleep loss, smoke is one of the more mechanistically concrete examples.
What the Evidence Can and Cannot Say Yet
The strongest direct sleep-architecture evidence still comes from animal models. That is a real limitation. Rodent sleep is not human sleep, exposure chambers are not bedrooms, and a controlled 1-hour exposure does not capture a week of intermittent smoke, home filtration, medication use, alcohol, sleep apnea, or a child waking in the next room.
Still, animal models are useful when they measure the intermediate biology that human survey studies often cannot: EEG sleep stages, HRV-related autonomic changes, blood pressure responses, inflammatory signaling, and controlled exposure timing. Human wildfire studies, by contrast, often have the advantage of lived reality but the disadvantage of mixed causes. Evacuation stress, property loss, trauma, heat, noise, and smoke can arrive together.
| Pathway | What changes during sleep | How strong the sleep-specific evidence is |
|---|---|---|
| Airway irritation | More coughing, congestion, airway resistance, snoring risk, and micro-arousals | Biologically strong; sleep-apnea evidence is associative, not proof of causation |
| Autonomic activation | Less parasympathetic dominance, more cardiovascular activation, disrupted NREM and REM cycling | Strongest direct support from the 2025 controlled EEG rodent study |
| Possible neuroinflammation | Potential effects on sleep-wake regulation through inflammatory or central nervous system pathways | Plausible and emerging for wildfire smoke; better established in other pollution contexts |
The calibrated conclusion is therefore neither alarmist nor dismissive. Wildfire smoke can plausibly and directly degrade sleep quality through airway irritation, sympathetic activation, and possibly neuroinflammatory effects. The most compelling current evidence shows that smoke exposure can alter measured sleep architecture in animals, while the human picture is likely more variable because exposure, health status, indoor air conditions, and psychological stress differ so much from one person to another.
If smoke-season sleep disruption persists after the air clears, or if it comes with wheezing, chest tightness, loud snoring, witnessed pauses in breathing, morning headaches, palpitations, or unusual daytime sleepiness, it is no longer just a bad night to explain away. A practical next step is to sort the pattern: insomnia, breathing symptoms, circadian disruption, anxiety, medication effects, or a possible sleep disorder. A self-triage guide for adults is built for that narrower question.
References
- Rentschler et al., Particle and Fibre Toxicology, 2025
- Association of Air Pollution and Sleep Disordered Breathing in the Multi-Ethnic Study of Atherosclerosis, PMC
- Research Contract 19RD005 Final Report, California Air Resources Board
- Martin et al., Frontiers in Environmental Health, 2023
- Climate Change Worsens Wildfire Smoke, Climate Central, 2025






Comments
Join the discussion with an anonymous comment.