When someone says they are not sleeping well, the useful question is not “How do I sleep better?” but “What pattern is this?” In U.S. survey data, 14.5% of adults reported trouble falling asleep most days or every day and 17.8% reported trouble staying asleep; a separate AASM survey found that 12% of Americans said they had been diagnosed with chronic insomnia [1][2]. That is enough common ground to justify a triage approach instead of another generic sleep checklist.

Start with the pattern, not the tips
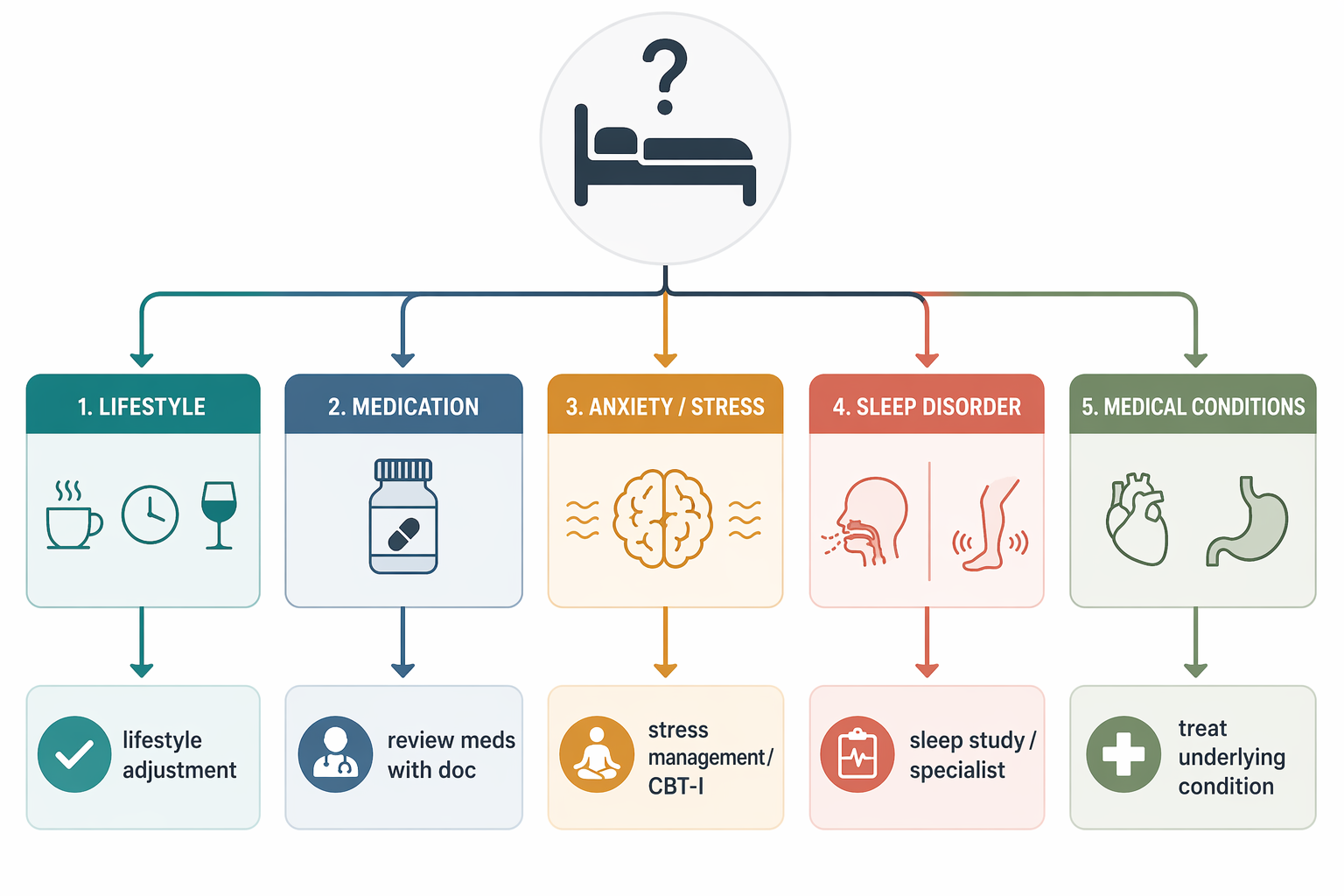
The first pass is simple: match the complaint to the clue that changes the next step. If the clue is obvious, the first move is usually a targeted change or a medication review. If the clue points to breathing, leg sensations, pain, reflux, or a long-running pattern, the right move is a clinician visit rather than more sleep hygiene.
| Bucket | Clues that fit | Most useful next move |
|---|---|---|
| Timing or lifestyle | Caffeine later in the day, alcohol near bedtime, late meals, long naps, drifting sleep schedule | Change one variable first and track whether sleep onset, awakenings, or morning refreshment changes |
| Medication effect | Sleep got worse after a new drug, a dose change, or an over-the-counter cold remedy | Review the medication list and timing with a clinician or pharmacist |
| Anxiety or stress | Racing thoughts, bedtime dread, repeated clock-checking, awake but mentally “on” | Address the sleep-stress loop directly; consider CBT-I or mental-health support |
| Sleep apnea | Loud snoring, gasping, witnessed pauses, morning headache, unrefreshing sleep | Book a sleep evaluation |
| Restless legs | Creepy-crawly leg sensations, urge to move, worse at rest, relief with movement | Ask about RLS and possible iron or medication causes |
| Medical condition or circadian shift | Pain wakes you, reflux after late meals, repeated nighttime urination, burning feet, sleep window drifting earlier | Look for the underlying condition instead of adding more sleep tips |
A useful shortcut: if the problem started after a change you can actually name, that change matters. If the problem has no obvious trigger but has become frequent, the threshold matters more than the story you tell yourself about it.
When the pattern is probably lifestyle
This is the easiest branch to test because it is reversible. Later caffeine, alcohol close to bedtime, late meals, naps that run long, and a sleep schedule that keeps moving all make sleep less stable. The point is not to start a perfection project; it is to isolate one likely cause and see whether the sleep problem moves with it. If you already know the barrier is timing or habits, a barrier-matching guide such as How to Fall Asleep Based on What's Actually Keeping You Awake is more useful than another general list of sleep tips.
Medication changes deserve their own check
Medication-related insomnia is easy to miss because the original reason for the prescription fades from memory. If sleep got worse after starting or changing an antidepressant, beta blocker, corticosteroid, stimulant, or even a cold remedy, the timing may be doing the talking. Write down the exact name, dose, and time of day you take it, then compare that timeline with when the sleep change began. That usually tells you more than guessing.
Do not stop a prescribed medicine on your own just because sleep feels off. The useful move is to bring the medication list to the prescriber or pharmacist and ask whether the timing, dose, or formulation could be part of the problem.
Stress and anxiety can both cause and follow bad sleep
This branch matters because people often treat it as a mood problem alone. Stress can keep the brain in a higher-alert state at night, and repeated short sleep can then make anxiety harder to regulate the next day [4]. The pattern usually looks like mental activation more than physical discomfort: lying there with a loop of unfinished tasks, clock-watching, waking with dread, or only falling asleep after exhaustion finally takes over. If that sounds familiar, sleep and anxiety need to be handled as a coupled problem, often with cognitive behavioral therapy for insomnia [5].
For readers who want the mechanism rather than the triage, How Better Sleep Improves Your Mental Health is the cleaner next stop.
Sleep apnea is a different problem from insomnia
Snoring by itself is noisy; snoring with gasping, witnessed pauses, choking, or persistent daytime sleepiness is a different signal. The sleeper may not notice the pauses at all; a bed partner often does. Morning headache, dry mouth, and unrefreshing sleep add weight to the suspicion. A crowded airway or a smaller jaw can also raise concern. This is not a branch for self-correction alone, because the issue is breathing interruption during sleep, not a lack of willpower at bedtime.
Restless legs has its own signature
Restless legs syndrome is often described in odd language because people struggle to name it: creepy-crawly, pulling, buzzing, or an urge to move the legs. The clue is not just discomfort. It is the combination of rest-triggered symptoms, evening worsening, and relief with movement. That pattern can delay sleep even when the bedroom is quiet and the schedule is regular. If the complaint is actually in the legs rather than the mind, another sleep-hygiene pass will not solve it.
Other medical clues are worth taking seriously
- Pain that wakes you or keeps you from settling points toward chronic pain rather than primary insomnia.
- Burning, sour taste, or symptoms that worsen after lying down point toward reflux.
- Repeated nighttime urination with weak stream or hesitancy points toward a urinary issue such as BPH.
- Burning or tingling in the feet or hands points toward neuropathy.
- A sleep window that shifts earlier with age can reflect circadian change more than a sleep disorder.
These clues do not automatically mean the sleep problem is “just medical” or “just age.” They mean the sleep complaint has a different target, and the target should not be hidden inside generic advice.
When to stop self-triaging
If symptoms happen at least 3 nights a week for at least 3 months, they meet the usual chronic insomnia threshold [3]. That does not prove one cause, but it does mean the problem is no longer a temporary rough patch. Earlier appointment makes sense if the pattern includes snoring with gasping or witnessed pauses, restless-leg symptoms, a clear medication trigger, substantial daytime impairment, or a medical symptom such as pain, reflux, or urinary waking that keeps repeating.
If the picture fits chronic insomnia after the obvious contributors are addressed, cognitive behavioral therapy for insomnia is the usual first-line treatment, and many patients improve with it [5].
Choose the next move
If the clue is timing or routine, make one targeted change and track it. If the clue is a medication, review the prescription list and timing with the prescriber. If the clue is breathing, leg sensations, pain, reflux, urinary waking, or a 3-month pattern on 3 or more nights each week, make the appointment. Once the bucket is clear, the next step is clearer too: lifestyle-branch readers can use The Evidence-Based Sleep Improvement Hierarchy or Sleep Tips Ranked by Evidence Strength — A Tiered Guide; anxiety-driven readers can move into How Better Sleep Improves Your Mental Health.
References
- “Trouble Falling Asleep or Staying Asleep Most Days or Every Day Among Adults: United States, 2020” — CDC National Center for Health Statistics
- “Survey Shows 12% of Americans Have Been Diagnosed With Chronic Insomnia” — American Academy of Sleep Medicine
- “Insomnia Diagnosis” — Sleep Foundation
- “How Sleep Deprivation Affects Your Mental Health” — Columbia University Department of Psychiatry
- “Cognitive Behavioral Therapy for Insomnia (CBT-I)” — Cleveland Clinic






Comments
Join the discussion with an anonymous comment.