During a tropical storm, the sleep-aid question is not “What will knock me out?” It is “If my phone alarms at 3 a.m., will I wake up, understand it, and act?” That standard immediately rules out some familiar over-the-counter choices. A sleep aid that leaves you groggy into the next morning can be a poor match for a night when forecasts shift, water rises, power fails, or someone in the house needs help.
The clearest concern is the half-life of first-generation antihistamines. Diphenhydramine can have a half-life of about 4 to 8 hours, while doxylamine can run about 6 to 12 hours, which means the sedating effect can still matter when daylight cleanup, evacuation decisions, generator use, or driving become the problem in front of you.[1]

The storm-night safety standard
A sleep aid used during tropical storm disruption has to pass a different test than a routine insomnia product. It should help you rest without blunting your ability to wake, hear alerts, read instructions, drive if ordered to leave, operate basic equipment, check on another person, or recognize that conditions have changed.
That does not mean everyone should stay awake all night. Sleep deprivation also makes people slower and more reactive. But during active storm conditions, lighter sleep is sometimes the safer target. A few broken hours, with alerts still able to reach you, may be a better outcome than chasing a normal night with a drug that is still working when the road outside is flooded.
For the mechanics of why wind, pressure changes, noise, threat monitoring, and disrupted routines disturb sleep, see How Tropical Storms Affect Sleep Through Four Pathways. The short version for choosing a sleep aid is practical: if the environment may require a fast response, avoid anything likely to slow recognition and decision-making.
How common sleep aids compare when alertness matters
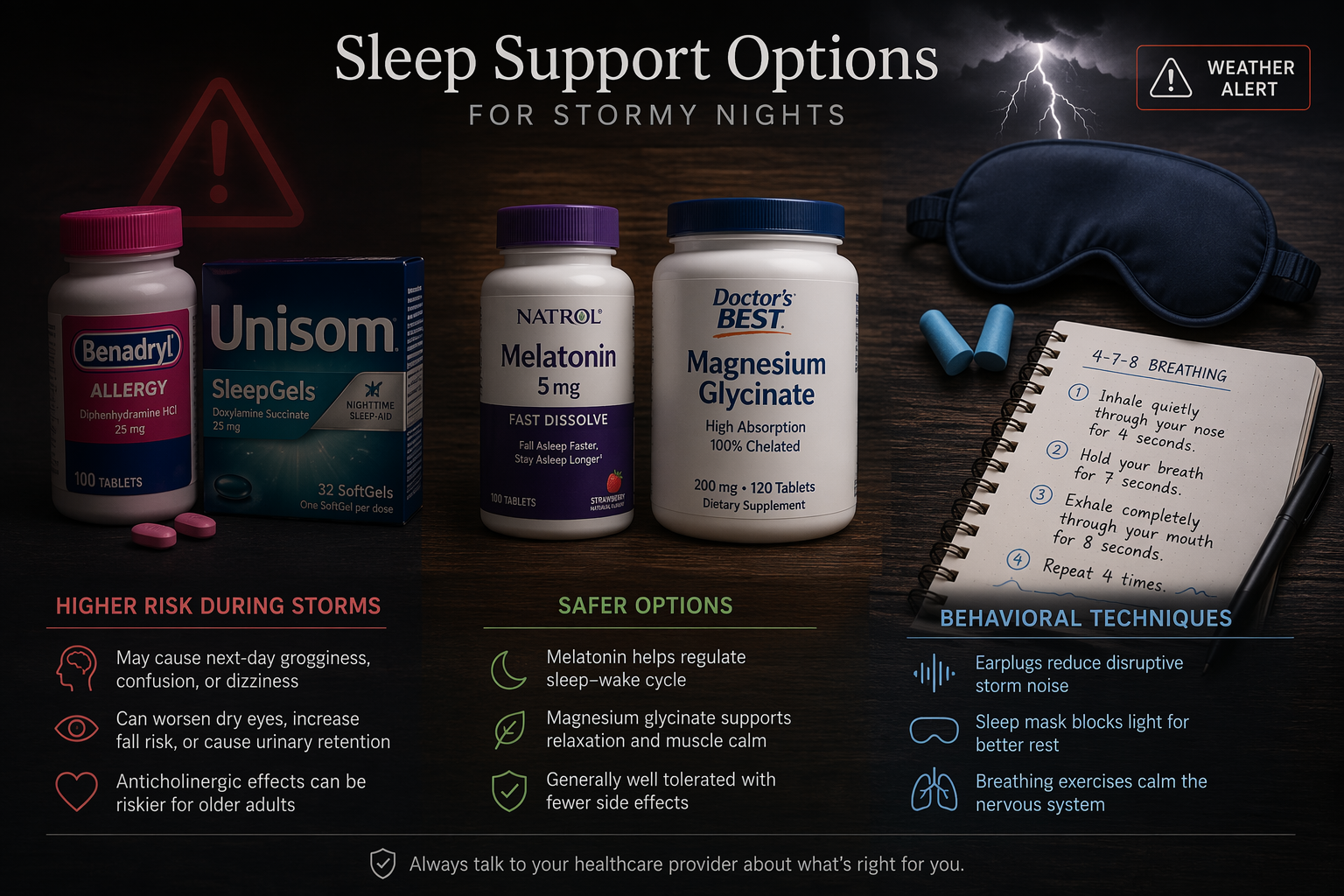
| Option | Storm-night fit | Main concern |
|---|---|---|
| Diphenhydramine | Poor during active storm conditions | Residual sedation can overlap with emergency decisions; half-life about 4 to 8 hours |
| Doxylamine | Usually worse fit than diphenhydramine during uncertainty | Longer half-life window, about 6 to 12 hours, makes next-day impairment harder to plan around |
| Melatonin | Often a safer option when used cautiously | Product label accuracy and dose selection matter; it is not an emergency sedative |
| Magnesium glycinate | Reasonable for some people before the storm, less useful as a same-night rescue | Sleep benefit is modest and not immediate for everyone |
| Behavioral and noise strategies | Best first-line choice during active storm conditions | They require practice and may not fully overcome panic or loud conditions |
Diphenhydramine and doxylamine: the “non-habit-forming” problem
Diphenhydramine is the sedating antihistamine found in many nighttime pain relievers and allergy-style sleep products. Doxylamine is the sedating ingredient in some Unisom products. Both are often marketed in ways that sound reassuring because they are not the same as prescription hypnotics. In a storm, that reassurance misses the main point.
The problem is not only whether these drugs are “habit-forming.” The problem is whether they are still affecting you when you need to wake cleanly. With diphenhydramine’s 4- to 8-hour half-life and doxylamine’s 6- to 12-hour half-life, a dose taken at 10 p.m. can still be relevant the next morning, especially with doxylamine.[1]
That residual window matters during tropical weather. Morning is often when people discover roof leaks, blocked roads, spoiled refrigeration, fallen limbs, or a changed forecast track. It is also when a person may need to drive, call relatives, decide whether to leave, or handle equipment that should not be handled while foggy.
Older adults need extra caution. The National Council on Aging warns that antihistamines such as diphenhydramine can be risky for older adults because of side effects including confusion, dizziness, and increased fall risk.[2] Those concerns are not theoretical when the hallway is dark, the floor is wet, and the power is out.
Doxylamine deserves particular caution in this setting. Its longer half-life window makes it harder to choose a “safe” bedtime dose when the emergency timeline is uncertain. If conditions are deteriorating, if alerts are possible, or if you may need to drive the next morning, doxylamine is a bad fit. For a deeper review outside the storm context, see Doxylamine as a Sleep Aid: Safety, Dosage, and Who Should Avoid It and Is Unisom a Safe Sleep Aid?.
Melatonin: safer for wakefulness, but not a free pass
Melatonin is usually a better storm-night fit than sedating antihistamines because it is not meant to chemically overpower wakefulness. It supports circadian timing rather than acting like a blunt sedative, and it is not associated with respiratory depression in the way some stronger sedatives can be. That distinction matters for people who need to remain responsive.
Dose still matters. Many adults do better starting low, often in the 0.5 to 3 mg range, rather than assuming a higher dose will produce safer or better sleep. If you already know melatonin leaves you groggy, gives you vivid dreams, or makes you feel off the next morning, a storm night is not the time to experiment. For dose-specific guidance, see the Melatonin Dosage Guide.
Product choice is the irritating part. Melatonin supplements are not all reliably labeled, and gummy products in particular have raised label-accuracy concerns. If you use melatonin during storm season, choose a product you have tolerated before, avoid stacking it with alcohol or other sedating substances, and do not test a new brand on the night alerts are possible. For formulation differences, see How to Choose Between Melatonin Gummies, Capsules, and Liquids.
Magnesium glycinate: modest help, not a rescue tool
Magnesium glycinate can be reasonable for some people who already use it and tolerate it well. Its advantage during storm season is that it is not designed to knock you out. Its limitation is just as important: the sleep benefit is modest, and it is not a reliable same-night fix for fear, wind noise, or a weather radio going off.
That makes magnesium more useful before the storm than during the worst hours. If it is part of your normal evening routine, it may be fine to continue unless your clinician has told you otherwise. If you have kidney disease, take medications that interact with minerals, or are already using several supplements, check safety before adding it. For a fuller evidence review, see Magnesium Glycinate for Sleep: Evidence, Dosage, Timing, and Safety.
Behavioral and noise tools: the best active-storm starting point
Behavioral tools have one major advantage during severe weather: they do not put a drug between you and the next alert. CBT-I is an evidence-based approach for insomnia, and its components can be adapted for an acute storm night even when a full treatment program is not the goal.[3]
- Cognitive shuffling: pick a neutral word, then list unrelated words or images for each letter. The aim is not to solve the storm; it is to give the brain a low-stakes track to follow.
- 4-7-8 breathing: inhale for 4, hold for 7, exhale for 8. If breath holds feel uncomfortable, shorten the counts and keep the exhale longer than the inhale.
- Progressive muscle relaxation: tense and release one muscle group at a time, starting with the feet or hands. Keep it gentle; this is not a workout.
- Worry containment: write down the next check-in time, the alert source you will trust, and the action threshold that would get you out of bed.
Anxiety-specific storm guidance also emphasizes preparation, limiting repeated forecast checking, and using calming strategies before panic peaks.[4] That does not make the storm less real. It keeps the brain from treating every gust as a separate decision.
Noise control should reduce sharp sound peaks without cutting you off from warnings. Soft foam earplugs, a fan, white noise, brown noise, or rain sounds can help, but keep emergency alerts on a device that is charged, loud enough, and close enough to wake you. If you use earplugs, test whether you can still hear your chosen alert tone before you go to bed.
Choose by storm phase, not by product strength
A sleep aid that is acceptable two nights before landfall may be a bad choice while bands are moving through. The safer way to decide is to match the aid to the phase of the storm.
Before the storm: preserve your baseline
Before conditions become active, the goal is to avoid arriving exhausted. Use the lowest-risk tools first: a consistent bedtime, dimmer lights, packed supplies, charged devices, and a written plan for when you will check forecasts. If you already use melatonin or magnesium glycinate without next-day effects, this is the phase where they make the most sense.
This is also when to remove decision friction. Put shoes, glasses, medications, flashlight, power bank, water, and keys where you can reach them. Set emergency alerts before you are tired. If you use a CPAP, confirm the backup-power plan while you are awake enough to troubleshoot it.
During active storm conditions: avoid sedating antihistamines
During active wind, flooding risk, tornado watches, evacuation uncertainty, power instability, or caregiving duties, skip diphenhydramine and doxylamine. This is the wrong moment to trade awareness for deeper sleep.
Use a layered setup instead. Keep the phone or weather radio audible. Use one noise-reduction method that you have already tested. Set a check-in time if conditions are concerning but not immediately dangerous. Use cognitive shuffling or progressive relaxation after that check-in rather than continuing to refresh radar in bed.
If you take melatonin during active conditions, keep the dose conservative and use only a product you already know. Do not combine it with alcohol, cannabis, sedating antihistamines, benzodiazepines, opioids, or other substances that may impair waking or breathing. If your situation requires you to be the designated driver, generator operator, medical-equipment monitor, or only adult in the home, non-drug methods are the safer choice.
Some storm-sleep advice describes accepting only 3 to 5 hours of broken sleep during the most active conditions, but that figure is experiential guidance rather than a controlled trial.[5] It is still a useful frame: storm sleep does not have to look normal to be successful. The safer win may be short sleep blocks with intact alertness.
After the storm: watch for delayed impairment
After the worst weather passes, the temptation is to finally take the strongest thing in the cabinet. Be careful. The post-storm period often brings the most hands-on work: clearing debris, checking on neighbors, dealing with insurance photos, driving around outages, or making decisions about food, water, and repairs.
If you are no longer on alert, not driving, not operating equipment, and not responsible for someone else overnight, your usual sleep routine may be reasonable. But a long-acting antihistamine can still make the next morning harder. If you need recovery sleep, prioritize a dark room, hydration, cooler temperature if possible, a nap window, and a return to regular timing before reaching for sedating OTC products.
Special situations that change the answer
No sleep aid is universally safe during a storm. The same product can be low-risk for one adult on a quiet pre-storm night and a poor choice for another person who may need to evacuate, care for a child, or respond to a medical device alarm.
- Older adults: avoid first-generation antihistamines unless a clinician has specifically advised otherwise; confusion, dizziness, and falls become more dangerous in power outages or wet conditions.[2]
- CPAP users: do not use a sedating aid to “sleep through” power uncertainty. Confirm battery backup, outlet access, mask fit, and what you will do if power fails.
- Parents and caregivers: if you are the person who must hear alerts, children, oxygen equipment, a sump pump, or a relative calling for help, choose non-drug methods first.
- Pregnancy: do not self-select a storm-night sleep aid because a product is sold over the counter. Ask your clinician, especially before using doxylamine or combining products.
- Medication interactions: avoid stacking sedating sleep aids with alcohol, opioids, benzodiazepines, muscle relaxants, cannabis, some antidepressants, or other products that already cause drowsiness.
People with severe insomnia or storm panic may need individualized medical help. That is different from grabbing an antihistamine because it is available. If tropical systems reliably trigger panic, it is worth planning with a clinician before hurricane season rather than improvising during a warning.
What disaster sleep research can and cannot tell us
The strongest disaster-sleep studies often come from severe events, not ordinary tropical-storm nights. For example, the American Academy of Sleep Medicine reported high rates of insomnia symptoms among survivors after a major earthquake, with 94% of participants experiencing insomnia symptoms in the study it summarized.[6] That does not mean a tropical storm produces the same rate of insomnia.
Still, the mechanisms scale down. Wind noise, pressure changes, loss of routine, threat monitoring, and uncertainty can all disturb sleep before conditions reach catastrophic levels. Cleveland Clinic notes that barometric pressure changes can trigger headaches in some people, which is one way weather can become physically disruptive rather than merely annoying.[7]
That is why the sleep-aid decision should stay grounded in the actual night in front of you. A mild rainy evening, a tropical storm watch, a tornado warning embedded in a rain band, and a post-landfall cleanup morning are not the same sleep environment.
A practical storm-night protocol
- Check the role you must play overnight: sleeper only, caregiver, driver, medical-device user, equipment operator, or alert monitor.
- If alerts, evacuation, flooding, power instability, caregiving duties, CPAP dependence, pregnancy, older age, or medication interactions are in play, avoid diphenhydramine and doxylamine.
- Use non-drug tools first: audible alerts, tested earplugs or noise masking, breathing, cognitive shuffling, progressive muscle relaxation, and a written next-check time.
- If using melatonin, keep it low-dose, familiar, and uncombined with other sedating substances.
- If using magnesium glycinate, treat it as part of a normal routine, not as a same-night emergency sedative.
- Accept lighter sleep if conditions are active. The safer goal is to rest while remaining reachable by the next important warning.
If the night is uncertain, choose the aid that leaves the least residue on your judgment. In tropical weather, that is usually not the strongest OTC sleep aid. It is the method that lets you wake up clear enough to do the next right thing.
References
- Doxylamine vs. Diphenhydramine: GoodRx
- Natural Sleep Remedies: National Council on Aging
- Cognitive Behavioral Therapy for Insomnia: NIH/PMC
- Hurricane Season Is Here: How to Reduce Your Anxiety: Anxiety and Depression Association of America
- Hurricane Preparedness and Sleep: Amerisleep
- Disturbed Sleep Linked to Mental Health Problems in Natural Disaster Survivors: American Academy of Sleep Medicine
- Barometric Pressure Headache: Cleveland Clinic






Comments
Join the discussion with an anonymous comment.