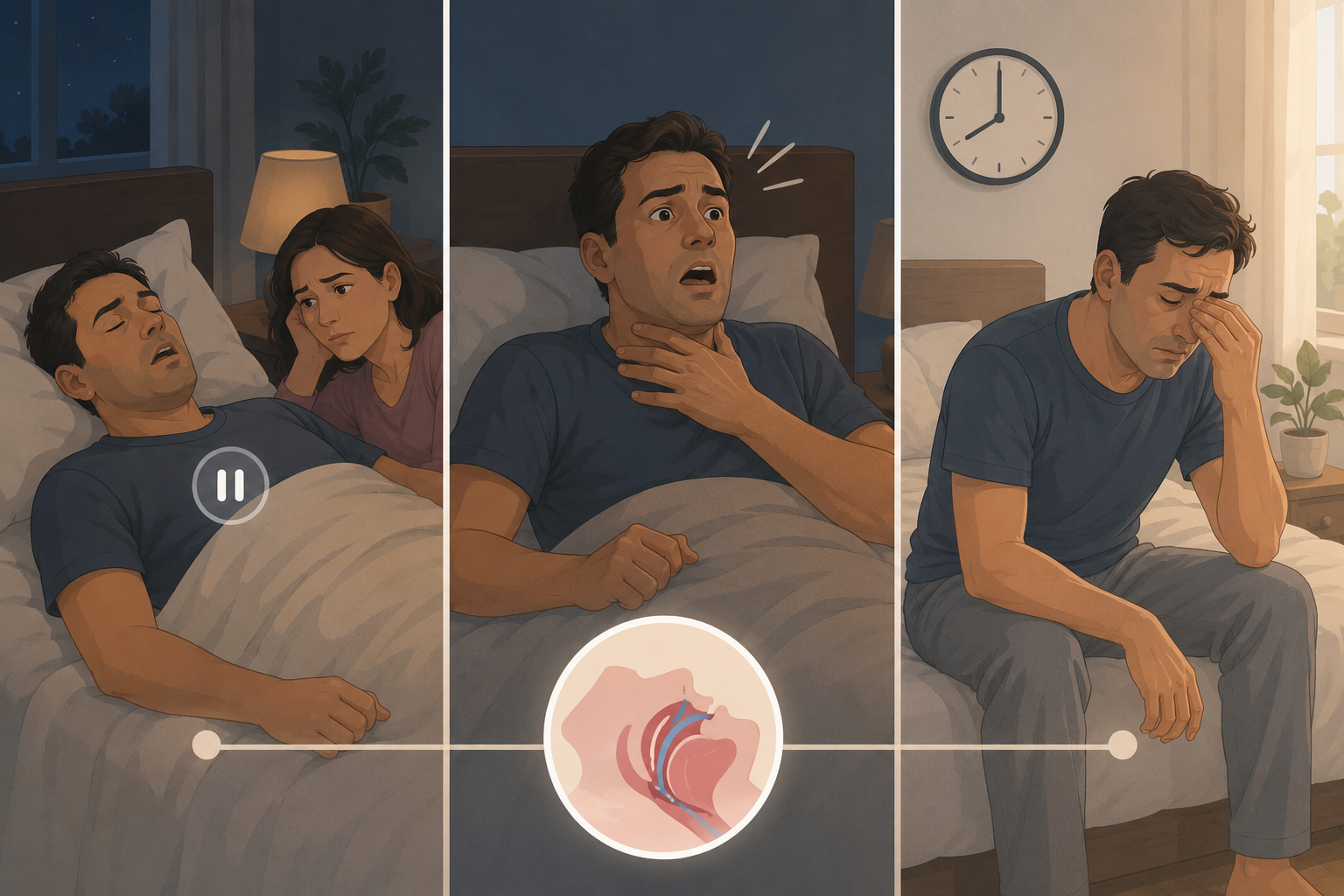
The first useful clue often comes from the person who is not asleep. They hear the snoring change rhythm, then stop. A few seconds later, the sleeper snorts, gasps, coughs, or jerks awake, and in the morning may remember none of it. That is the uncomfortable household moment behind most searches for snoring vs sleep apnea symptoms: one person feels accused of making noise, while the other is trying to describe breathing that looked wrong.
Snoring by itself is common. About 25% to 50% of adults snore regularly, and most regular snorers do not have sleep apnea.[1] That matters, because every snore does not need to become a medical emergency. But obstructive sleep apnea is also widely missed: the American Academy of Sleep Medicine reports that nearly 30 million adults in the U.S. have obstructive sleep apnea, with about 23.5 million cases undiagnosed.[2] The useful question is not “Do I snore?” It is “Does the snoring come with breathing disruption or daytime impairment?”
The Core Difference Is Breathing, Not Noise
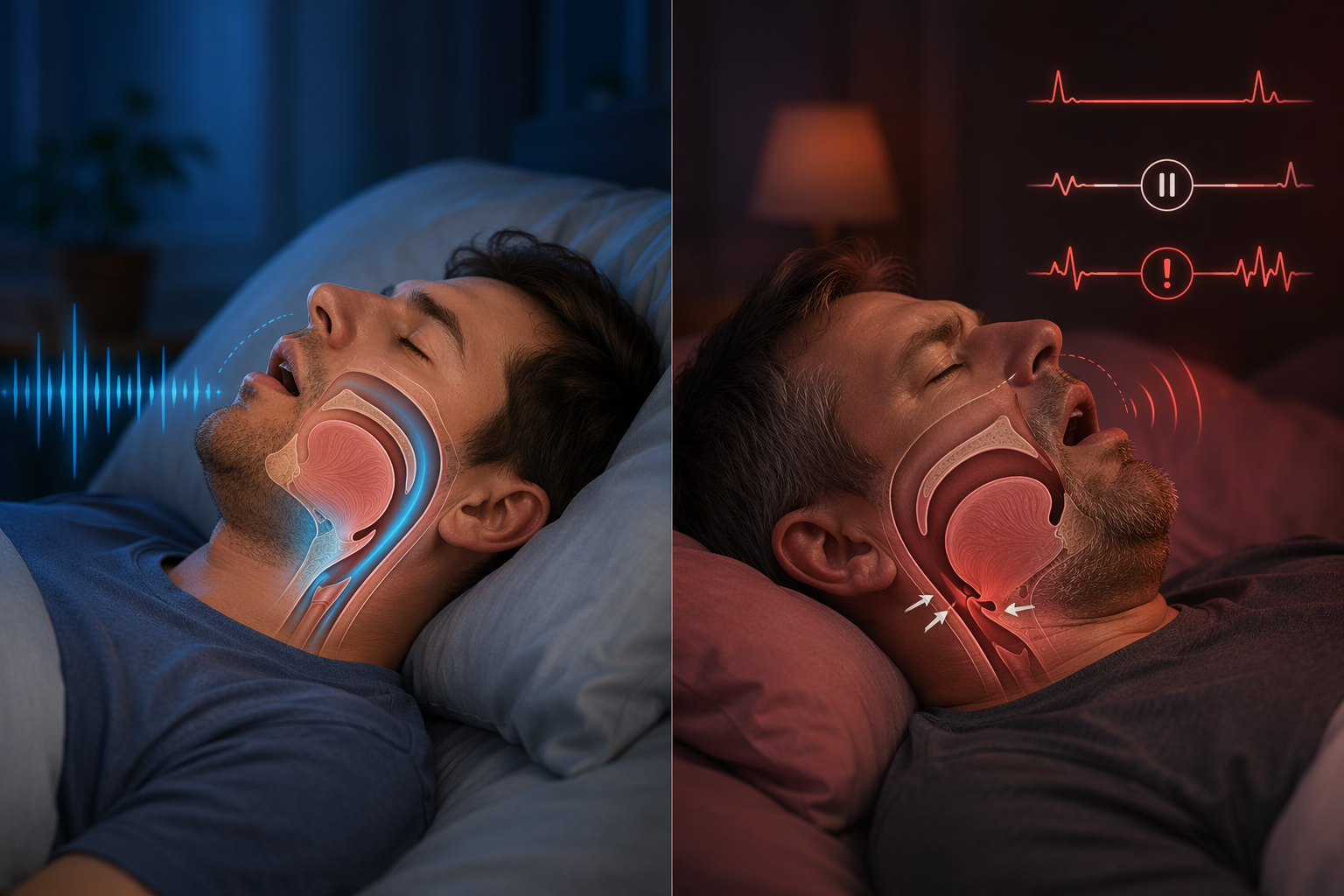
Simple snoring is sound from a narrowed or vibrating upper airway. Obstructive sleep apnea is repeated breathing disruption during sleep. The airway partly or fully collapses, breathing drops or pauses, sleep can fragment, oxygen may fall, and the person may wake repeatedly without forming a clear memory of waking.
Clinically, obstructive sleep apnea is not diagnosed by how annoyed a partner is. It is measured by breathing events. The apnea-hypopnea index, or AHI, counts apneas and hypopneas per hour of sleep. OSA can be diagnosed when breathing pauses or reductions lasting at least 10 seconds occur at least 5 times per hour with symptoms, or at 15 or more events per hour even without symptoms.[3]
That definition is why symptom triage has to look past volume. Loud snoring can raise suspicion; Johns Hopkins Medicine notes that the louder snoring becomes, the greater the chance of sleep apnea.[4] But loudness alone does not prove that breathing stopped, oxygen dropped, or sleep was repeatedly interrupted.
The Three Symptoms That Most Strongly Shift the Question
A bed partner’s report should not be treated as background noise. In a 2021 AASM survey, 70% of Americans who shared a bed said their partner snored, while 48% did not know the symptoms of sleep apnea.[2] That gap is exactly where people get stuck: the person with the best evidence may not know what the evidence means.
1. Witnessed Breathing Pauses
A pause is different from a loud snore. The concerning pattern is a stretch where breathing seems to stop, often followed by a snort, gasp, or body movement. The sleeper may insist nothing happened because the brain often does not store these brief arousals as memorable awakenings.
This is one place where the observer’s account deserves real weight. A person cannot reliably report what their airway did while they were asleep. If someone repeatedly sees breathing stop, the question has moved beyond ordinary snoring and into “should this be tested?”
2. Gasping, Choking, or Waking With a Jolt
Gasping or choking during sleep suggests the body is responding to restricted breathing. Some people describe it as waking in a panic, waking with a dry throat, or suddenly sitting up to catch their breath. The episode may be brief, but its meaning is not the same as steady, uncomplicated snoring.
A single bad night with congestion or alcohol is not the same as a recurring pattern. Repeated gasping or choking, especially when paired with snoring or witnessed pauses, is a strong reason to ask a clinician about sleep apnea evaluation.
3. Daytime Sleepiness Despite Enough Time in Bed
Seven or eight hours in bed does not guarantee seven or eight hours of restorative sleep. Sleep apnea can repeatedly pull the brain out of deeper sleep without producing full awakenings that the person remembers. The result may be morning exhaustion, dozing during quiet activities, poor concentration, irritability, or needing far more caffeine than usual to function.
Daytime sleepiness is especially important when the person’s schedule appears adequate. If short sleep, shift work, a new baby, or another obvious cause explains the exhaustion, that context matters. But unexplained sleepiness in a regular snorer should not be brushed aside as laziness, aging, or “just bad sleep.”
Symptom-by-Symptom: Ordinary Snoring vs Sleep Apnea
| Symptom or clue | More consistent with ordinary snoring | More concerning for sleep apnea |
|---|---|---|
| Sound pattern | Steady vibration or rumbling without obvious breathing stops | Snoring interrupted by silence, then snorting, gasping, choking, or sudden movement |
| Breathing pauses | No one observes pauses in breathing | A partner or household member sees breathing stop or become irregular |
| Morning state | Generally refreshed if sleep time was adequate | Wakes unrefreshed despite enough time in bed |
| Daytime function | No major sleepiness, dozing, or concentration problems | Excessive daytime sleepiness, impaired focus, or unplanned naps |
| Loudness | May be loud, especially with congestion, alcohol, or sleeping on the back | Loud snoring plus pauses, gasping, choking, or daytime impairment |
| Blood pressure context | No known hypertension pattern connected to sleep complaints | High blood pressure or resistant hypertension alongside snoring or sleepiness |
Morning headaches, dry mouth, sore throat, restless sleep, and frequent nighttime urination can also appear with sleep apnea, but they are less decisive on their own. They become more meaningful when they cluster with witnessed pauses, gasping, or unexplained daytime sleepiness.
Why “I Snore, But I Feel Fine” Can Be Tricky
Some people with sleep apnea do not feel dramatically sleepy, or they have adjusted to feeling tired for so long that it seems normal. Others sleep alone and never hear the most important clue. That is why symptom judgment is strongest when it combines what the sleeper feels with what someone else observes.
Simple snoring can also change over time. SleepApnea.org describes snoring and obstructive sleep apnea as part of a spectrum of airway obstruction, with simple snoring producing no oxygen drops, no sleep fragmentation, and no daytime functional impairment.[1] If the pattern shifts from harmless noise to breathing disruption or daytime dysfunction, it deserves a new look.
High Blood Pressure Raises the Stakes
Blood pressure does not diagnose sleep apnea, but it changes how casually snoring should be treated. The AASM reports that 30% to 40% of adults with high blood pressure also have sleep apnea.[2] A global burden review also reports that up to 83% of patients with resistant hypertension may have undiagnosed obstructive sleep apnea.[5]
The highest-risk outcome data apply to people with more severe, untreated disease, not to every person who snores. In the Wisconsin Sleep Cohort, untreated severe sleep-disordered breathing was associated with a 3.8-fold higher risk of all-cause mortality over 18 years.[6] That finding should not be used to frighten someone with occasional uncomplicated snoring. It should be used to avoid ignoring repeated breathing pauses, choking episodes, or sleepiness in someone who may have clinically significant OSA.
If high blood pressure is part of the picture, especially if it is hard to control, it is worth reading more about treating high blood pressure when you have sleep apnea and bringing the sleep symptoms into the same medical conversation.
When Snoring Is More Likely to Be Benign
Snoring is more likely to be simple snoring when it is not accompanied by witnessed pauses, gasping, choking, or daytime impairment. It may worsen with nasal congestion, alcohol before bed, sleeping on the back, or airway anatomy. Those factors can narrow the airway enough to create noise without necessarily producing repeated obstructive events.
- The snoring is steady rather than stop-start.
- No one has seen breathing pauses or choking.
- The person wakes reasonably refreshed when sleep time is adequate.
- There is no unexplained daytime sleepiness or impaired function.
- The snoring clearly tracks with temporary triggers such as congestion or alcohol.
In that situation, it is reasonable to monitor the pattern and reduce obvious aggravating factors. The important word is monitor. A snoring pattern that becomes louder, more irregular, or paired with daytime symptoms is no longer the same problem.
When a Sleep Study Becomes the Next Step
A sleep study becomes the right next question when symptoms suggest repeated obstruction rather than harmless vibration. That does not mean the diagnosis is already settled. It means the pattern is strong enough that guessing from symptoms is no longer adequate.
- Ask about evaluation if someone has witnessed breathing pauses during sleep.
- Ask about evaluation if snoring is followed by gasping, choking, or abrupt awakenings.
- Ask about evaluation if daytime sleepiness persists despite adequate time in bed.
- Ask about evaluation if snoring or sleepiness occurs alongside high blood pressure, especially resistant hypertension.
- Ask about evaluation if a validated risk screen suggests high risk for moderate-to-severe OSA.
Testing may be done with a home sleep apnea test or an in-lab polysomnogram, depending on symptoms, medical history, and clinician judgment. If cost or test type is the immediate barrier, compare home sleep test vs lab study cost before assuming one route is out of reach.
Where STOP-Bang Helps, and Where It Does Not
STOP-Bang is a screening questionnaire, not a diagnosis. It asks about snoring, tiredness, observed apneas, blood pressure, body mass index, age, neck circumference, and gender. A score of 5 or higher is generally considered high risk for moderate-to-severe obstructive sleep apnea.[7]
It is useful as a bridge between vague concern and a medical conversation. It is less useful when treated as a final answer. Lower scores can still miss people, and the gender item can reduce scores for women in a way that may understate risk. At lower thresholds, STOP-Bang can also produce false positives, meaning some people will screen as at risk without ultimately having clinically significant OSA.
The Important Exception: Sleep Apnea Without Classic Snoring
A snoring-first framework can fail, especially for women. A review cited in the global burden literature reports that up to 40% of women with obstructive sleep apnea may not report snoring.[5] That does not mean snoring is unimportant. It means the absence of reported snoring should not cancel out other symptoms such as insomnia-like sleep complaints, fatigue, morning headaches, mood changes, or unexplained daytime impairment.
Anyone trying to interpret a less stereotypical symptom pattern should use the sleep apnea symptom checklist for women rather than relying only on loud snoring and witnessed apneas.
What Wearables Can and Cannot Tell You
Consumer sleep trackers, oxygen trends, and breathing-disturbance features can raise suspicion. They can also help someone notice a repeated pattern worth discussing. But they cannot confirm obstructive sleep apnea, determine an official AHI, or replace a home or in-lab sleep study.
If a device flags breathing disturbances, treat that as a signal to gather better information, not as a diagnosis. For a deeper comparison, see why your sleep tracker is not a sleep study.
What to Do While You Are Deciding
If symptoms look benign, start with observation and reversible triggers: congestion, alcohol close to bedtime, sedating medications that should be reviewed with a clinician, and back-sleeping if the snoring is clearly position-related. If sleep apnea is possible, these steps may reduce noise or events for some people, but they should not delay evaluation when red flags are present.
For practical interim ideas, read about the best sleeping position for sleep apnea or a severity-based guide to home remedies for sleep apnea. If a diagnosis later shows mild OSA, treatment does not always mean one single path; CPAP alternatives for mild sleep apnea may become part of the discussion.
The decision point is simple enough to keep on the nightstand: steady snoring without pauses, choking, or daytime impairment can usually be watched and managed. Snoring with witnessed breathing pauses, gasping or choking, unexplained daytime sleepiness, or relevant blood pressure concerns deserves medical evaluation. Symptoms can strongly separate ordinary snoring from probable sleep apnea, but only formal testing can confirm the diagnosis.
References
- Snoring vs. Sleep Apnea, SleepApnea.org.
- Is it more than a snore?, American Academy of Sleep Medicine, 2021.
- Obstructive sleep apnea, Mayo Clinic.
- 4 Signs You Might Have Sleep Apnea, Johns Hopkins Medicine.
- The global burden of obstructive sleep apnoea, PMC, 2025.
- Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort, Sleep, 2008.
- STOP-Bang Score for Obstructive Sleep Apnea, Sleep Foundation.






Comments
Join the discussion with an anonymous comment.