If CPAP treats obstructive sleep apnea, it is reasonable to ask why the blood pressure medication list did not disappear. The short answer is that CPAP can help blood pressure, sometimes meaningfully, but it usually does not lower it enough to replace hypertension treatment. For most adults with both obstructive sleep apnea and hypertension, the safer plan is coordinated rather than sequential: treat the airway problem consistently, measure the blood pressure response honestly, and keep using antihypertensive medication when the numbers still require it.
That answer may feel unsatisfying if you were hoping one diagnosis would explain everything. It is still the answer that best fits the evidence. CPAP is the cornerstone therapy for obstructive sleep apnea, but average blood pressure reductions are modest: roughly 2–7 mmHg systolic and 2–5 mmHg diastolic, with larger effects in some groups, especially people with resistant hypertension, more severe OSA, and stronger nightly adherence, often defined in studies as at least 4 hours per night.[1]

| Part of the plan | What it is meant to do | What to expect |
|---|---|---|
| CPAP or another OSA therapy | Reduce airway collapse, oxygen drops, and nighttime nervous-system surges | Can lower blood pressure, but usually by a modest amount |
| Antihypertensive medication | Control blood pressure to the target set by your clinician | Often still needed even when CPAP is used well |
| Weight and metabolic treatment when appropriate | Address shared drivers such as obesity and cardiometabolic risk | May improve OSA severity and blood pressure in selected patients |
| Follow-up and home measurements | Show whether the combined plan is working | Especially important if blood pressure remains high on several medications |
For a broader explanation of symptoms, testing, and treatment options, start with this obstructive sleep apnea guide or the Sleep Apnea FAQ. Here, the narrower question is the sleep apnea and high blood pressure connection: what changes in the body, what CPAP can realistically change, and what clinicians usually add when blood pressure remains above goal.
Why Sleep Apnea Can Keep Blood Pressure High
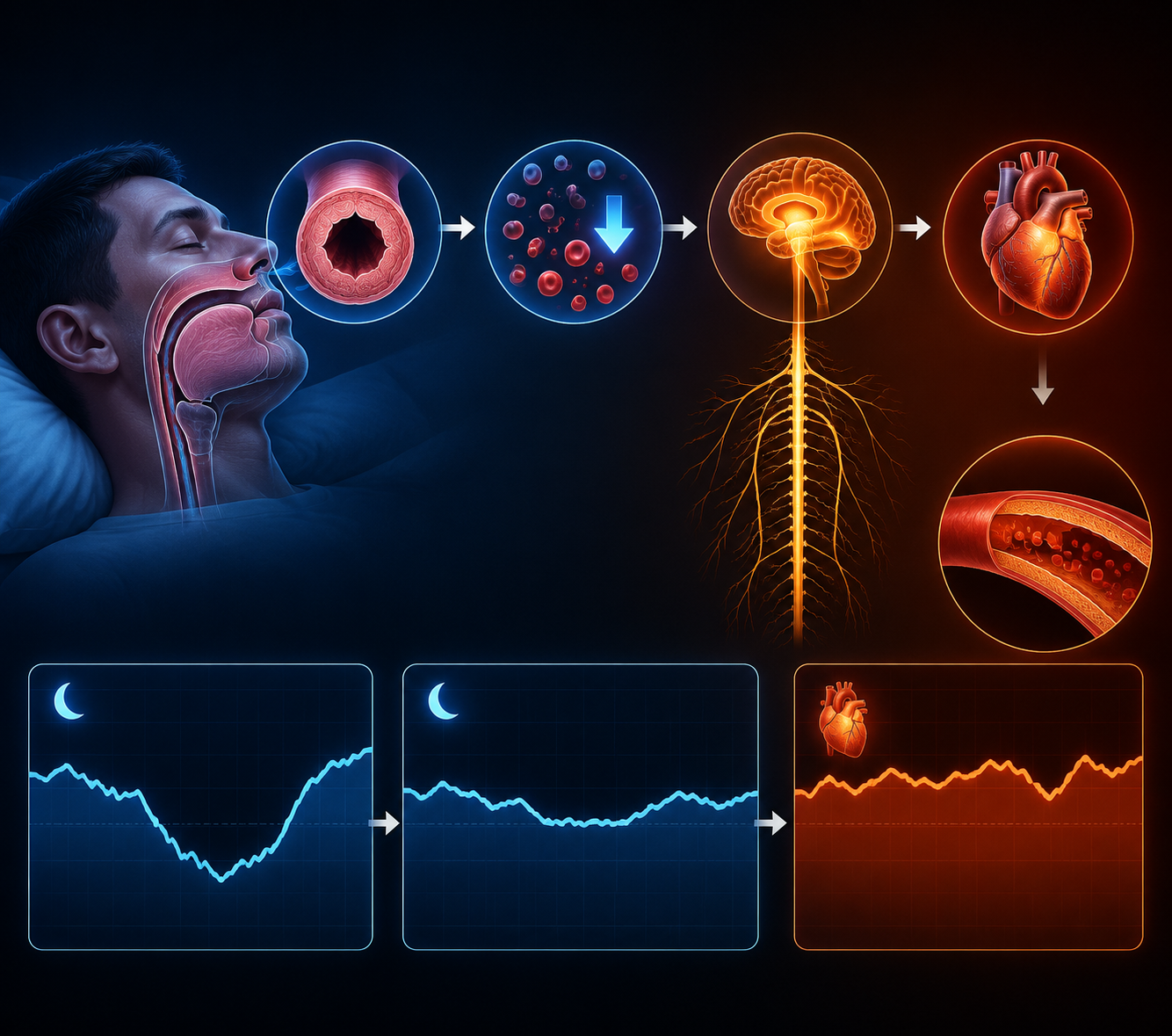
Obstructive sleep apnea repeatedly narrows or closes the upper airway during sleep. Each event can drop oxygen levels, fragment sleep, and trigger sympathetic nervous system activation—the same “fight or flight” system that raises heart rate and tightens blood vessels. Over a night, that pattern can keep the cardiovascular system from getting the quieter period it is supposed to have.
One useful sign is the nighttime blood pressure pattern. Many people without this problem have a normal nocturnal “dip,” often described as a 10–20% blood pressure drop during sleep. Sleep Foundation and SleepApnea.org both describe untreated OSA as commonly associated with a non-dipping pattern, with one reported figure placing non-dipping at 84% among untreated OSA patients.[2][3]
This does not mean OSA is the only cause of hypertension. The causal picture is mixed: some cohort evidence supports OSA as an independent cause, while other large observational work has found that the association weakens after adjusting for body mass index. A careful way to say it is that obstructive sleep apnea can contribute to and worsen hypertension, especially at night and in patients whose blood pressure is already hard to control.
What CPAP Usually Does—and Does Not Do—for Blood Pressure
CPAP works on the airway problem directly. By holding the airway open, it reduces apnea and hypopnea events, improves oxygen stability, and lowers the repeated sympathetic surges that can push blood pressure upward. That physiologic logic is strong, and withdrawal data make it hard to dismiss: when CPAP is stopped, office systolic blood pressure has been reported to rise by 5.4 mmHg and home systolic blood pressure by 9.0 mmHg within one week.[1]
But preventing a rise is not the same as curing hypertension. Across studies, the average CPAP-related blood pressure reduction is usually in the modest range, about 2–7 mmHg systolic and 2–5 mmHg diastolic.[1] That can matter. A few millimeters of mercury can affect cardiovascular risk across populations, and for an individual near goal, it may be enough to change a treatment decision. For a patient starting at 156/94 mmHg, it is usually not enough by itself.
The difference between “helps” and “solves it” is where many patients get trapped. A person may use the machine, still have high readings, and conclude either that CPAP failed or that they failed. Neither conclusion is necessarily true. CPAP may be doing exactly what the evidence predicts—lowering pressure somewhat, reducing nighttime stress, and protecting against rebound when it is skipped—while medication is still needed to reach a safe blood pressure target.
Who tends to see larger blood pressure changes?
The average CPAP effect hides important differences. People with more severe OSA, better nightly adherence, and resistant hypertension tend to show larger reductions.[1] Resistant hypertension changes the stakes because it describes a blood pressure pattern that remains high despite multiple medications, or requires multiple medications to stay controlled. In that setting, missing OSA is not a small oversight.
A 2023 meta-analysis reported that people with OSA had 4.16 times higher odds of resistant hypertension. In patients with resistant hypertension, CPAP was associated with an average blood pressure reduction of −7.21 mmHg systolic and −4.99 mmHg diastolic.[4] That is still not a guarantee of medication-free control, but it is a large enough signal to justify treating OSA as part of the hypertension plan rather than as a separate sleep complaint.
Adherence deserves plain language here. A mask that sits unused on the nightstand cannot lower nighttime blood pressure. A mask that is worn only during the first part of the night may miss later REM-heavy sleep, when apnea can worsen for some people. If CPAP is uncomfortable, noisy, drying, or claustrophobic, that is not a character flaw; it is a treatment problem that should be adjusted. Mask refitting, pressure changes, humidification, and follow-up data downloads can matter as much as the prescription itself.
Adjunctive strategies can help some people use therapy better or reduce OSA severity, but they should not be quietly substituted for effective treatment when OSA is moderate to severe. If you are weighing comfort measures, see home remedies for sleep apnea, natural remedies for sleep apnea, and this discussion of whether home remedies can replace CPAP. Positional therapy may also be relevant for some patients, especially when apnea is worse on the back; this sleeping position guide explains that piece.
Why Blood Pressure Medication Often Stays in the Plan
Once CPAP is started, the next practical question is not whether medication is “still necessary” in the abstract. The question is what the blood pressure actually does after sleep therapy is being used consistently. If readings remain above the goal set by the clinician, antihypertensive treatment should not be delayed out of loyalty to CPAP.
Standard hypertension care still matters: accurate measurement, home readings when appropriate, kidney function and electrolyte monitoring, attention to diabetes and cardiovascular disease, and medication choices based on the whole patient. OSA adds another layer because sympathetic activation, fluid shifts, obesity, and nighttime blood pressure patterns may influence which drugs are most useful for a given person.
The ESADA cohort adds useful but not definitive clues. In that analysis, beta-blocker monotherapy was associated with lower systolic blood pressure in non-obese middle-aged males with OSA, and the combination of ACE inhibitor or ARB therapy with CPAP showed particularly strong blood pressure control.[1] Those findings should not be read as a universal prescribing rule. They are a signal for clinicians to consider OSA physiology alongside standard hypertension guidelines, not a reason for patients to request or stop a drug class on their own.
In clinic, the medication layer may look ordinary from the outside: an ACE inhibitor, ARB, calcium channel blocker, thiazide-type diuretic, beta-blocker, mineralocorticoid receptor antagonist, or other drug depending on the patient. The OSA-specific work is in the judgment behind the choice. Is the patient still non-dipping? Are morning readings high? Is there resistant hypertension? Is obesity, diabetes, kidney disease, or heart disease part of the same picture? Is the CPAP data showing adequate use, or is the blood pressure being judged before the sleep treatment has had a fair trial?
Patients should not be asked to reconcile this alone. A sleep specialist may focus on apnea-hypopnea index, leak, pressure, and mask tolerance. A primary-care clinician or cardiologist may focus on blood pressure targets, medication side effects, and cardiovascular risk. The plan works better when those conversations meet in the middle: CPAP data and home blood pressure logs should both be visible.
When Hypertension Is Resistant, OSA Deserves a Fresh Look
Resistant hypertension is the point where sleep apnea should move higher on the checklist. The 4.16-fold higher odds of resistant hypertension among people with OSA does not prove that OSA caused every case, but it is too strong to ignore.[4] If blood pressure remains high despite several medications, untreated or undertreated OSA can be one reason the plan keeps underperforming.
- Confirm the blood pressure pattern with proper office technique and home or ambulatory readings when appropriate.
- Check whether CPAP is being used long enough and whether leaks, pressure intolerance, or mask problems are limiting treatment.
- Review medications for dose, timing, side effects, and whether the regimen fits the patient’s other conditions.
- Look for other contributors, including kidney disease, high sodium intake, alcohol, interfering medications, and endocrine causes.
- Revisit weight, metabolic risk, and treatment options without treating weight loss as a moral test.
This is also where screening and diagnosis details matter. Wearables and consumer devices may flag breathing disturbances, but they do not replace a clinical diagnosis. If you are earlier in the process, this article on whether an Apple Watch can detect sleep apnea can help separate screening from diagnosis. Women may also have less classic symptom patterns, and this Sleep Apnea in Women FAQ covers that angle.
Where Newer Weight and Metabolic Therapies Fit
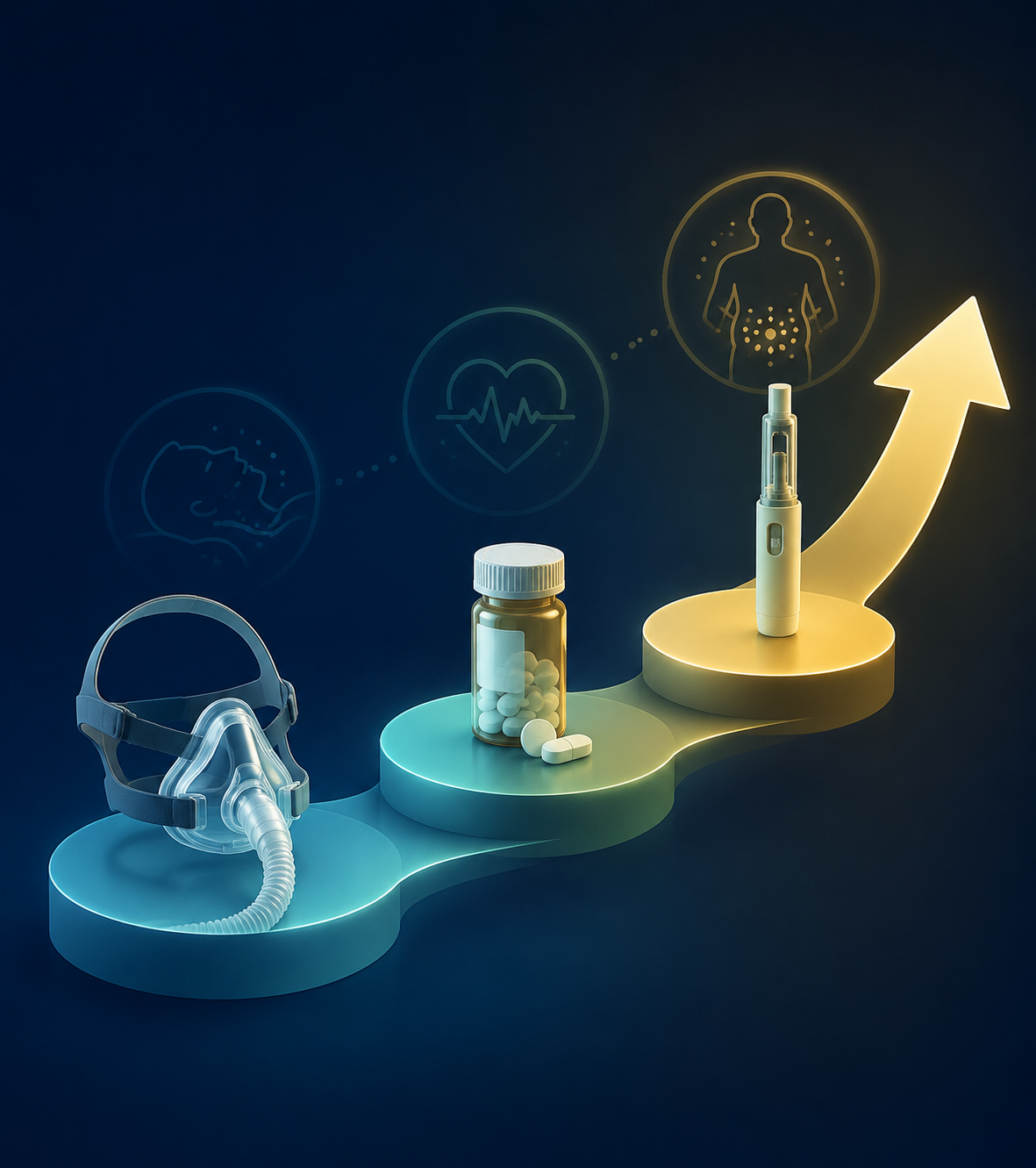
Newer metabolic medications are changing the conversation, but they do not erase the older sequence. CPAP remains the established airway therapy. Antihypertensive medication remains the direct blood pressure treatment. Weight-loss and metabolic therapies may be added when obesity or cardiometabolic disease is part of the same clinical picture.
Tirzepatide is the clearest example to watch in 2026. In the SURMOUNT-OSA phase 3 program, adults with obesity and moderate-to-severe OSA had reductions in apnea-hypopnea index, body weight, and systolic blood pressure; in the trial group not using CPAP, systolic blood pressure fell by −7.6 mmHg.[1] That is clinically important because it targets overlapping pathways rather than asking CPAP to carry the whole cardiovascular burden.
The boundaries matter. These data apply to adults with obesity and moderate-to-severe OSA in a phase 3 program, not to every person with snoring, mild OSA, or hypertension. Tirzepatide now has an FDA-approved context for moderate-to-severe OSA in adults with obesity, but it should not be described as a universal OSA treatment or a replacement for CPAP in patients who still need airway therapy.[1]
GLP-1 receptor agonists and related agents are attractive because they can affect weight, metabolic risk, OSA severity, and blood pressure at the same time. SGLT2 inhibitors are also being discussed in cardiometabolic care because many patients with hypertension, obesity, diabetes, kidney disease, or heart failure have overlapping risks. But the more useful question is not whether these drugs are “for sleep apnea” in a broad sense. It is whether a specific patient has an indication, can use the drug safely, can afford and tolerate it, and still needs CPAP or blood pressure medication after treatment begins.
A Practical Treatment Roadmap
The working order is simple enough, even when the details are not. Treat obstructive sleep apnea consistently. Do not assume CPAP will normalize blood pressure by itself. Measure the response with real blood pressure data. Keep or adjust antihypertensive medication when readings remain above goal. If hypertension is resistant, reassess CPAP effectiveness, medication strategy, and other secondary contributors rather than adding blame to the patient.
For adults with obesity and moderate-to-severe OSA, newer metabolic therapies may belong in the discussion, especially when weight, blood pressure, glucose, and cardiovascular risk are already part of the same visit. They should be placed where they belong: potentially powerful additions for selected patients, not shortcuts around airway treatment or standard hypertension care.
The patient who is wearing the CPAP mask and still taking blood pressure medicine has not misunderstood the assignment. That is often the assignment. The better question for the care team is whether each part of the plan is doing its job—and whether the sleep data, blood pressure readings, medication choices, and metabolic risks are being reviewed together.
References
- Management of hypertension in obstructive sleep apnea, Hypertension Research, 2024.
- How Sleep Apnea Affects Blood Pressure, Sleep Foundation.
- How Sleep Apnea Affects Blood Pressure, SleepApnea.org.
- Association between obstructive sleep apnea and resistant hypertension: a systematic review and meta-analysis, Frontiers in Medicine, 2023.






Comments
Join the discussion with an anonymous comment.